Case Report: Not all signet rings are of gastric origin: a case of lobular breast carcinoma metastatic to the stomach
Clinical Scorecard: Case Study: Identifying Non-Gastric Sources of Signet Ring Cells - A Lobular Breast Carcinoma Metastasis to the Stomach
At a Glance
Category Detail
Condition Invasive Lobular Carcinoma (ILC) with Gastric Metastasis Key Mechanisms Loss of E-cadherin facilitates diffuse infiltration; signet ring morphology mimics primary gastric cancer. Target Population Patients with a history of invasive lobular carcinoma. Care Setting Oncology and Gastroenterology
Key Highlights
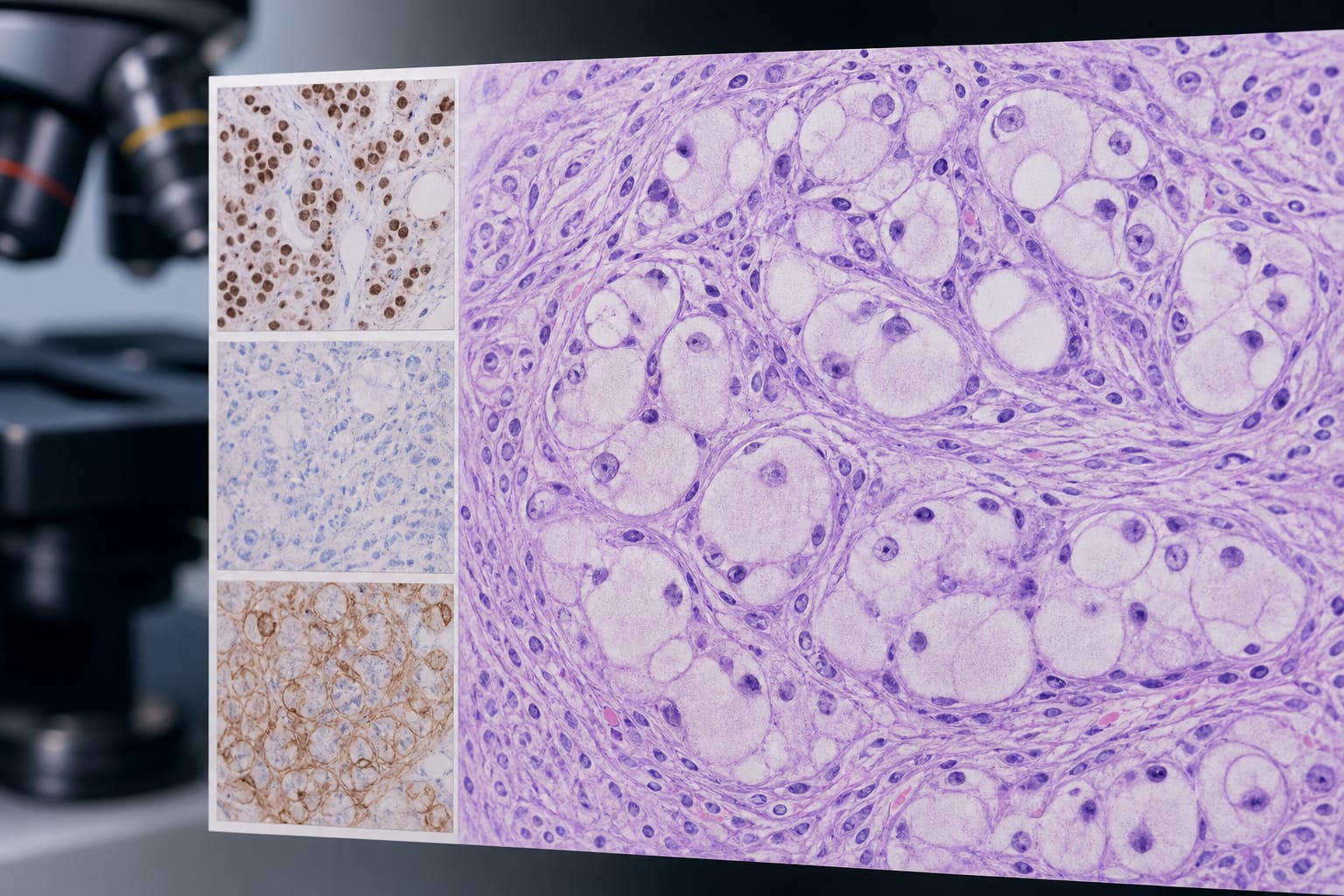
ILC accounts for 70% of gastric metastases from breast cancer despite being 10-15% of all breast cancers. Signet ring morphology in gastric biopsies can mislead diagnosis towards primary gastric cancer. An IHC panel with breast-lineage markers is crucial for accurate diagnosis. Guideline-Based Recommendations
Diagnosis
Utilize an IHC panel incorporating GATA3, TRPS1, and E-cadherin status. Management
Initiate systemic therapy based on histopathological findings and clinical symptoms. Monitoring & Follow-up
Monitor tumor markers and symptoms for disease progression. Risks
Misdiagnosis can lead to inappropriate surgery and delays in systemic therapy. Patient & Prescribing Data
Female patients with metastatic lobular breast carcinoma.
Weekly paclitaxel was initiated due to symptomatic gastric involvement.
Clinical Best Practices
Conduct thorough histopathological evaluations in patients with ILC presenting with GI symptoms. Consider the possibility of gastric metastasis in ILC patients with signet ring morphology. Related Resources & Content