Overall survival and progression-free survival in pediatric meningiomas: a systematic review and individual patient-level meta-analysis
By
Johannes Wach
Martin Vychopen
Alim Emre Basaran
Marcos Tatagiba
Roland Goldbrunner
Erdem Güresir
January 9, 2025
Clinical Scorecard: Survival Outcomes and Disease-Free Survival Rates in Pediatric Meningiomas: A Comprehensive Review and Meta-Analysis of Individual Patient Data
At a Glance
Category Detail
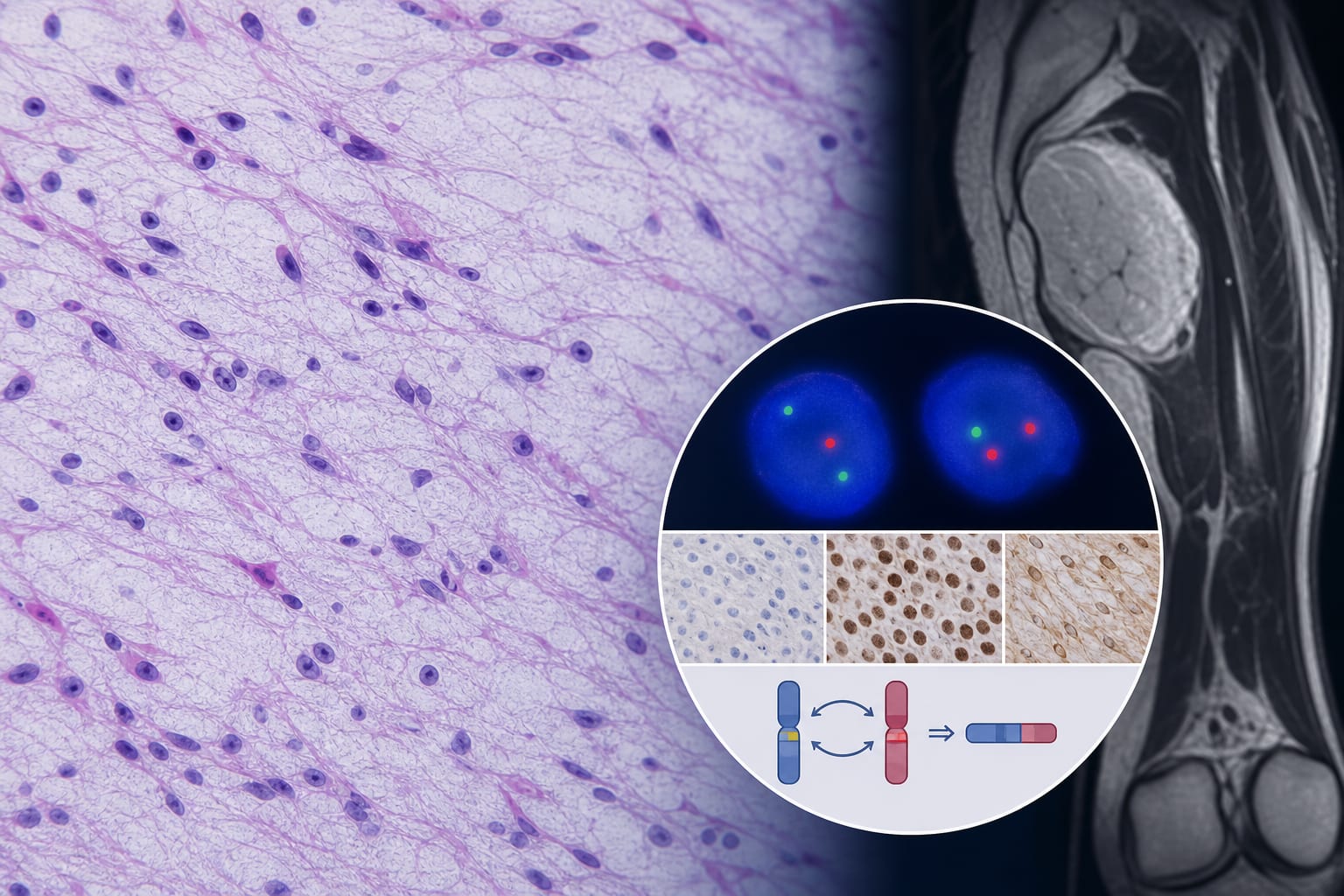
Condition Pediatric meningiomas (PMs), rare primary CNS tumors distinct from adult meningiomas Key Mechanisms Predominance of NF2 mutations; distinct genetic and histopathological profiles compared to adults Target Population Patients aged 21 years or younger with histopathologically confirmed cranial sporadic or NF-associated meningiomas Care Setting Specialized neuro-oncology and pediatric neurosurgery centers with longitudinal follow-up
Key Highlights
Pediatric meningiomas account for 1–5% of all meningiomas and differ clinically and molecularly from adult meningiomas. Progression-free survival (PFS) is significantly shorter in children diagnosed at ages 0–3 compared to older pediatric age groups. Neurofibromatosis type 2 (NF2) mutations predominate in PMs, with WHO grade and extent of resection influencing survival outcomes. Guideline-Based Recommendations
Diagnosis
Histopathological confirmation of cranial meningiomas in patients ≤21 years. Assessment of NF status, particularly NF2 mutation presence. Classification by WHO tumor grade (1, 2, or 3). Management
Aim for gross total resection (GTR, Simpson grades I-III) when feasible to improve progression-free survival. Consider adjuvant radiotherapy based on WHO grade and extent of resection, though data on chemotherapy are lacking. Tailor treatment strategies recognizing distinct pediatric tumor biology compared to adults. Monitoring & Follow-up
Longitudinal follow-up with progression-free survival and overall survival assessments. Use Kaplan–Meier survival analyses stratified by age, WHO grade, NF status, and extent of resection. Close monitoring especially in younger children (0–3 years) due to shorter PFS. Risks
Higher risk of progression in younger children (0–3 years). Potential for recurrence with subtotal resection (STR). Limited data on chemotherapy efficacy and dural attachment treatment. Patient & Prescribing Data
Pediatric patients aged 0–21 years with sporadic or NF-associated meningiomas
Gross total resection improves progression-free survival; adjuvant radiotherapy use varies by WHO grade; chemotherapy data insufficient
Clinical Best Practices
Perform comprehensive genetic and histopathological evaluation including NF2 mutation status. Prioritize gross total resection to maximize progression-free survival. Implement age-stratified risk assessment, recognizing younger patients have poorer PFS. Use multidisciplinary approaches integrating neurosurgery, radiotherapy, and genetic counseling. Maintain rigorous longitudinal follow-up with standardized survival outcome measures. References