Tislelizumab-induced distal renal tubular acidosis presenting with life-threatening hypokalemia: a case report
-
By
-
Jiaju Xu
-
Lidong Qin
-
Ping Wang
-
Zhen Liu
-
Lili Yang
-
Hongwei Zhang
-
Yanqiu Wang
-
Jiao Gao
-
Meishu Zhao
-
Kaili Zhang
-
June 11, 2026
-
Clinical Scorecard: Case Report of Life-Threatening Hypokalemia Due to Tislelizumab-Induced Distal Renal Tubular Acidosis
At a Glance
| Category | Detail |
|---|
| Condition | |
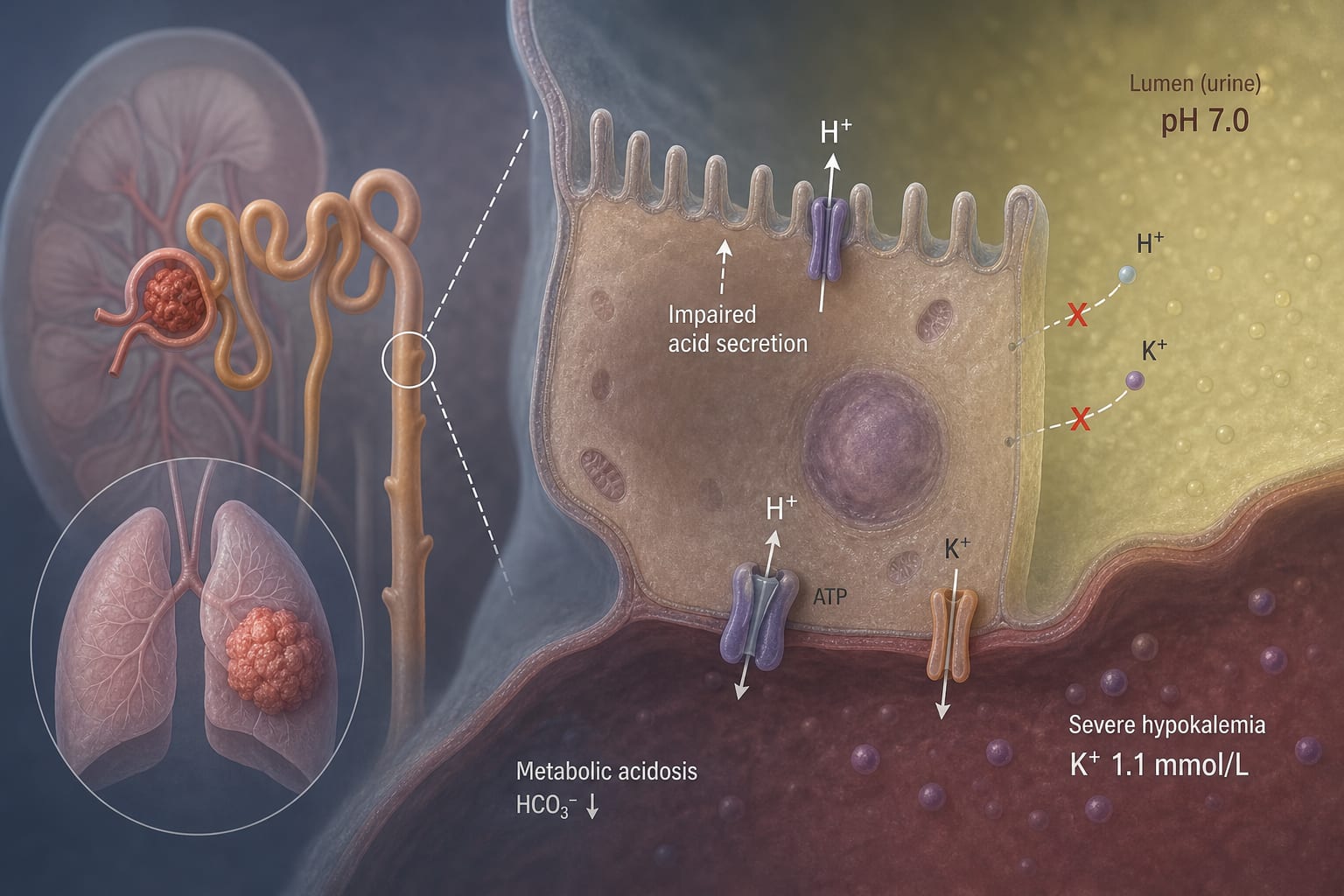
| Key Mechanisms | Impaired renal acidification leading to metabolic acidosis and refractory hypokalemia |
| Target Population | |
| Care Setting | |
Key Highlights
- Rare case of dRTA induced by tislelizumab in a patient with lung cancer
- Severe hypokalemia (1.1 mmol/L) despite aggressive potassium supplementation
- Diagnosis confirmed by urine pH and exclusion of other causes
- Treatment involved discontinuation of tislelizumab and administration of potassium citrate and prednisone
Guideline-Based Recommendations
Diagnosis
- Consider dRTA in patients with unexplained metabolic acidosis and hypokalemia during ICI therapy
- Use urine pH to differentiate dRTA from other causes of metabolic acidosis
Management
- Discontinue the offending immune checkpoint inhibitor
- Initiate treatment with potassium supplementation and consider corticosteroids
Monitoring & Follow-up
- Regularly monitor serum potassium and renal function during treatment
- Assess acid-base status and urine pH
Risks
- Potential for life-threatening hypokalemia and metabolic acidosis
Patient & Prescribing Data
Adult patients with lung cancer undergoing treatment with immune checkpoint inhibitors
Clinical Best Practices
- Maintain high suspicion for renal irAEs in patients on ICIs presenting with electrolyte imbalances
Related Resources & Content