Spontaneous brain abscess formation: challenge of a shifting pathogen spectrum over the last 21 years – a single center experience - Scorecard - MDSpire
Advertisement
Spontaneous brain abscess formation: challenge of a shifting pathogen spectrum over the last 21 years – a single center experience
Clinical Scorecard: Evolution of Pathogen Profiles in Spontaneous Brain Abscess Development: Insights from a 21-Year Single-Center Study
At a Glance
Category
Detail
Condition
Spontaneous intracerebral brain abscess
Key Mechanisms
Intracerebral abscess formation secondary to infections at other sites or cryptogenic origin; pathogen spectrum varies by anatomical source
Target Population
Adult patients (≥18 years) with spontaneous intracerebral abscesses
Care Setting
Neurosurgical department with imaging and surgical intervention capabilities
Key Highlights
Spontaneous brain abscesses represent a life-threatening condition with ~20% mortality despite modern treatment.
Most common pathogens include Streptococcus spp. and Staphylococcus spp., with increasing reports of gram-negative oral flora bacteria.
Surgical evacuation combined with empirical antibiotics (third-generation cephalosporins, vancomycin, metronidazole) is standard care.
Guideline-Based Recommendations
Diagnosis
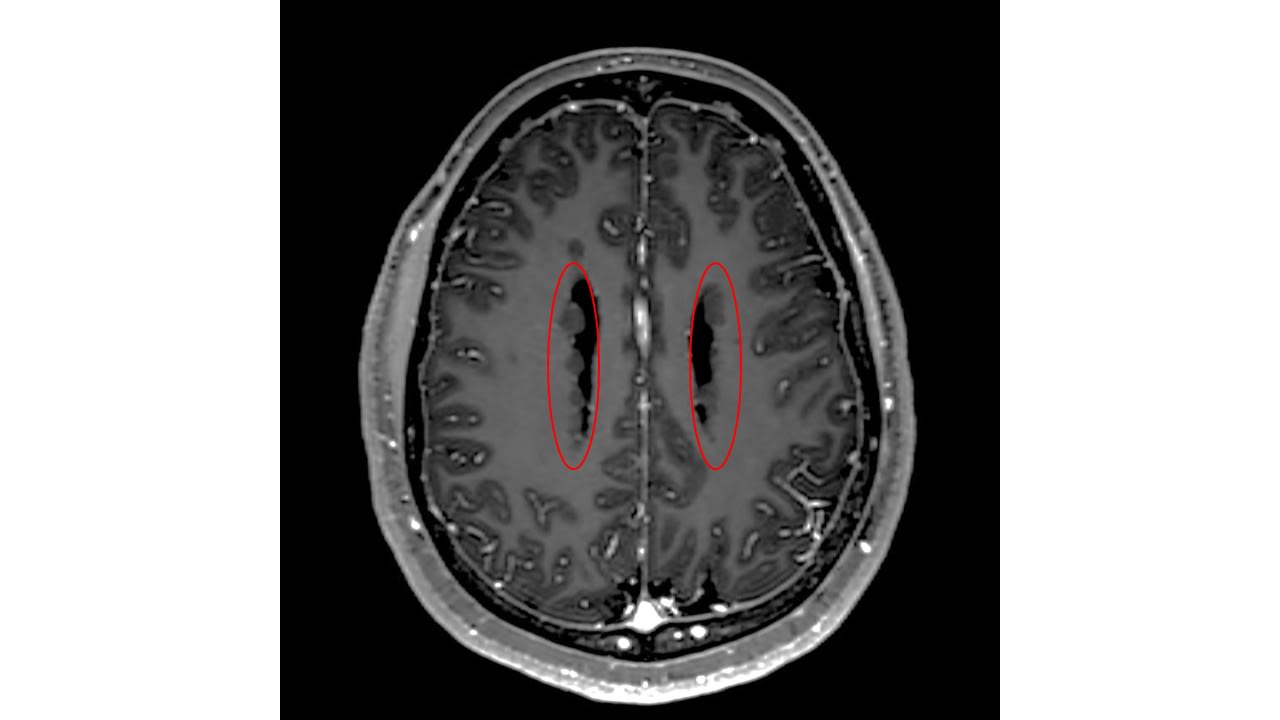
Confirm abscess via cranial imaging: CT scan and MRI with contrast focusing on T1-weighted and T2-weighted diffusion sequences (ADC).
Exclude postoperative abscesses and epidural/subdural collections for spontaneous abscess diagnosis.
Management
Perform surgical evacuation via open burr hole or stereotactic needle aspiration.
Administer empirical intravenous antibiotics combining third-generation cephalosporins, vancomycin, and metronidazole for anaerobic coverage.
Median antibiotic treatment duration is approximately four weeks.
Monitoring & Follow-up
Assess neurological status and clinical outcome using modified Rankin Scale (mRS) at follow-up.
Monitor for neurological sequelae, which occur in ~40% of patients post-treatment.
Risks
High mortality rate (~20%) despite treatment.
Neurological sequelae are common post-treatment.
Predisposing factors include immunodeficiency, malignancy, polytoxicomania, organ transplantation, liver cirrhosis, and other comorbidities.
Patient & Prescribing Data
65 adult patients with spontaneous intracerebral abscess treated surgically over 21 years
Surgical evacuation combined with a median 4-week intravenous antibiotic regimen resulted in 58 patients discharged alive; no significant correlation between antibiotic duration and outcome was observed.
Clinical Best Practices
Use combined imaging modalities (CT and MRI with contrast) for accurate diagnosis.
Exclude postoperative abscesses to focus on spontaneous cases.
Employ surgical evacuation promptly to reduce mortality and improve outcomes.
Use broad-spectrum empirical antibiotics covering gram-positive cocci and anaerobes.
Monitor patients closely for neurological sequelae and adjust management accordingly.
Consider patient comorbidities and immunodeficiency status in risk assessment.
by Luisa Mona Kraus, Manou Overstijns, Amir El Rahal, Simon Behringer, Klaus-Jürgen Buttler, Lukas Andereggen, Jürgen Beck, Oliver Schnell, Daniel Hornuss, Dirk Wagner, Debora Cipriani
Epilepsy remains a life-altering condition, particularly due to the unpredictable nature of seizures and their cumulative impact on cognition, independence and quality of life.