Clinical Scorecard: Incidence, Predictors, and Nationwide Cohort Analysis of Ongoing Opioid Use in ICU Survivors Post-Discharge
At a Glance
Category
Detail
Condition
New persistent opioid use among ICU survivors after hospital discharge
Key Mechanisms
Peri-ICU opioid exposure leading to prolonged opioid use post-discharge, influenced by demographic, socioeconomic, clinical, and treatment-related factors
Target Population
Adult ICU survivors who were opioid-naïve prior to ICU admission and survived at least 6 months post-discharge
Care Setting
Intensive care units and post-discharge outpatient settings within a nationwide healthcare system
Key Highlights
New persistent opioid use defined by opioid prescriptions filled in two distinct post-discharge windows: 1–90 days and 91–180 days.
Nationwide retrospective cohort study using South Korea’s NHIS database, capturing comprehensive demographic, clinical, and socioeconomic data.
Identification of predictors including mechanical ventilation, baseline comorbidity, socioeconomic status, and acute organ dysfunction during ICU stay.
Guideline-Based Recommendations
Diagnosis
Identify new persistent opioid use by monitoring outpatient opioid prescriptions in two post-discharge windows (1–90 days and 91–180 days).
Exclude inpatient opioid administrations to focus on community prescribing patterns.
Classify opioid potency to assess intensity of exposure (less potent vs. potent opioids).
Management
Consider risk factors such as mechanical ventilation, comorbidities, and socioeconomic status when planning post-ICU pain management.
Use cautious opioid prescribing strategies post-discharge to minimize prolonged use and potential harms.
Tailor analgesic regimens based on patient risk profiles and functional status.
Monitoring & Follow-up
Implement longitudinal prescription monitoring for at least six months post-discharge to detect persistent opioid use.
Assess patient functional status and comorbidity burden regularly to guide opioid tapering or alternative pain management.
Monitor for signs of opioid dependence, overdose risk, and impaired recovery.
Risks
Persistent opioid use post-ICU may lead to dependence, overdose, and impaired physical and psychological recovery.
Socioeconomic factors and baseline health status can increase risk of prolonged opioid use.
Potent opioid exposure post-discharge is associated with higher risk of ongoing use.
Patient & Prescribing Data
Opioid-naïve adult ICU survivors discharged alive and surviving at least 180 days post-discharge in South Korea.
Approximately 2–4% develop new persistent opioid use; potent opioids and socioeconomic and clinical predictors influence persistence; monitoring and tailored management are essential.
Clinical Best Practices
Use a standardized definition of new persistent opioid use based on prescription fills in two post-discharge windows.
Incorporate demographic, socioeconomic, and clinical predictors to identify high-risk patients.
Exclude inpatient opioid administration data to accurately capture community opioid use.
Classify opioid prescriptions by potency to assess risk and guide management.
Employ nationwide administrative data for comprehensive monitoring and research.
Ensure ethical oversight and data anonymization in retrospective pharmacoepidemiologic studies.
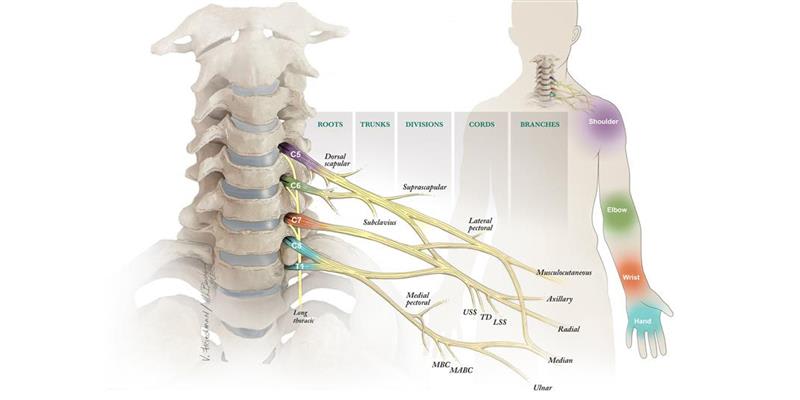
David Brogan, MD, MSc, and Christopher Dy, MD, MPH, who are pioneering new approaches to treating brachial plexus injuries, including those caused by high-velocity trauma such as motor vehicle accidents.