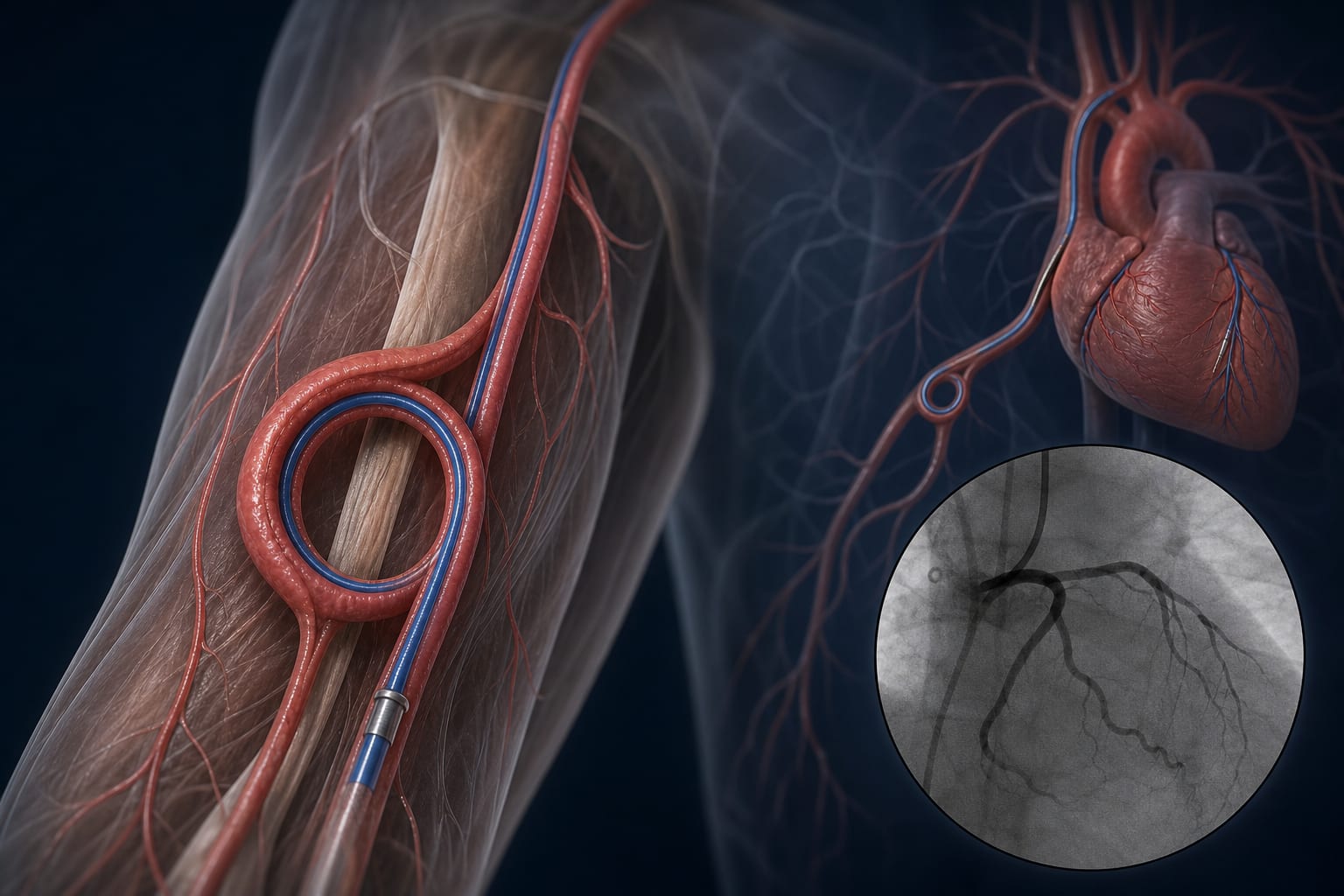
Case Report: When crossing is not enough: restoring functional access in an extreme brachial artery loop during primary PCI
-
By
-
Ali Hakan Konuş
-
Recep Polat
-
July 16, 2026
Clinical Scorecard: Case Study: Beyond Simple Traversal - Achieving Functional Access in an Extreme Brachial Artery Loop During Primary PCI
At a Glance
| Category | Detail |
|---|
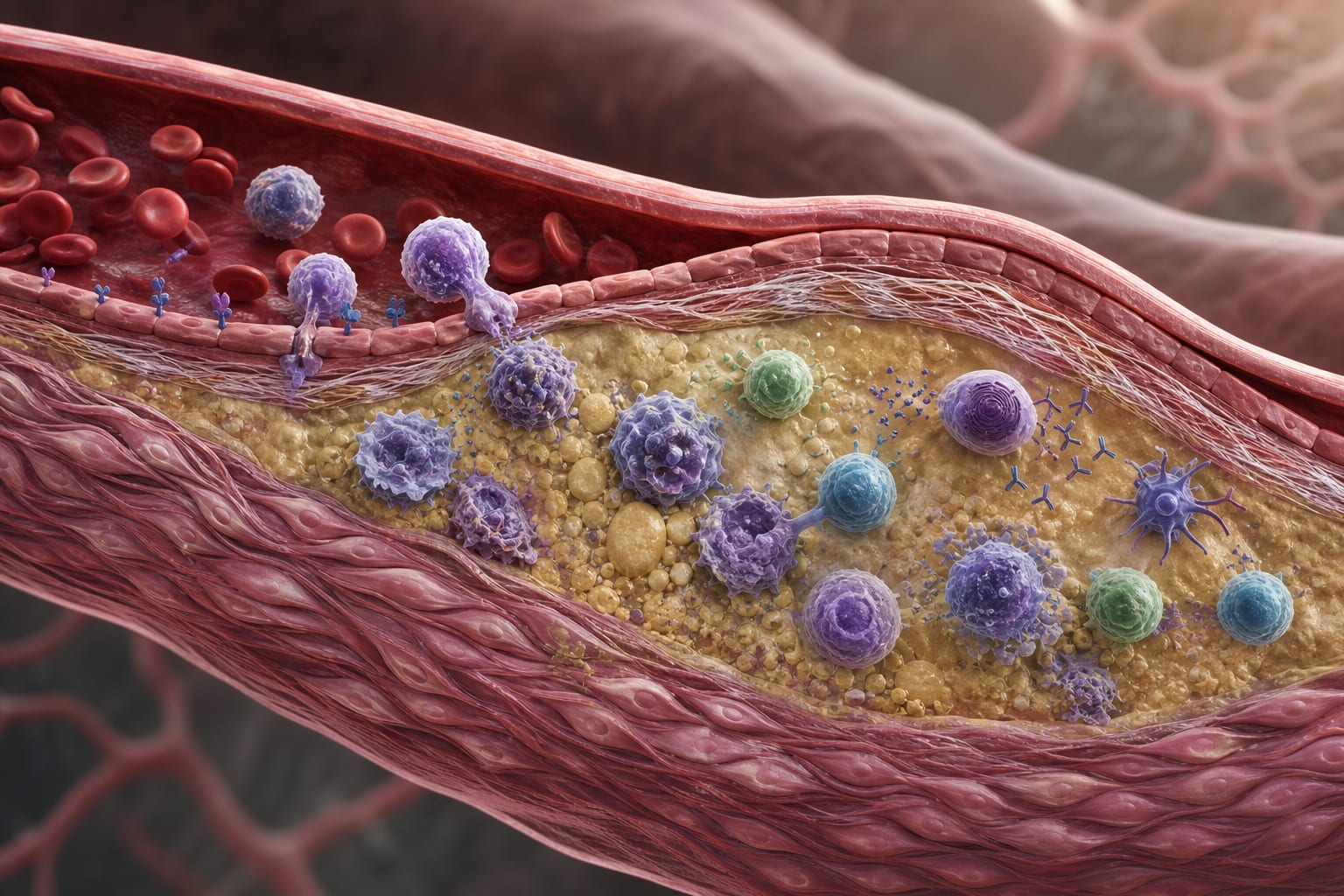
| Condition | Acute inferior ST-elevation myocardial infarction |
| Key Mechanisms | Distinction between successful traversal and functional access in tortuous arterial anatomy |
| Target Population | Patients undergoing primary PCI with extreme upper-limb arterial tortuosity |
| Care Setting | Catheterization laboratory |
Key Highlights
- Successful guidewire traversal does not guarantee functional access.
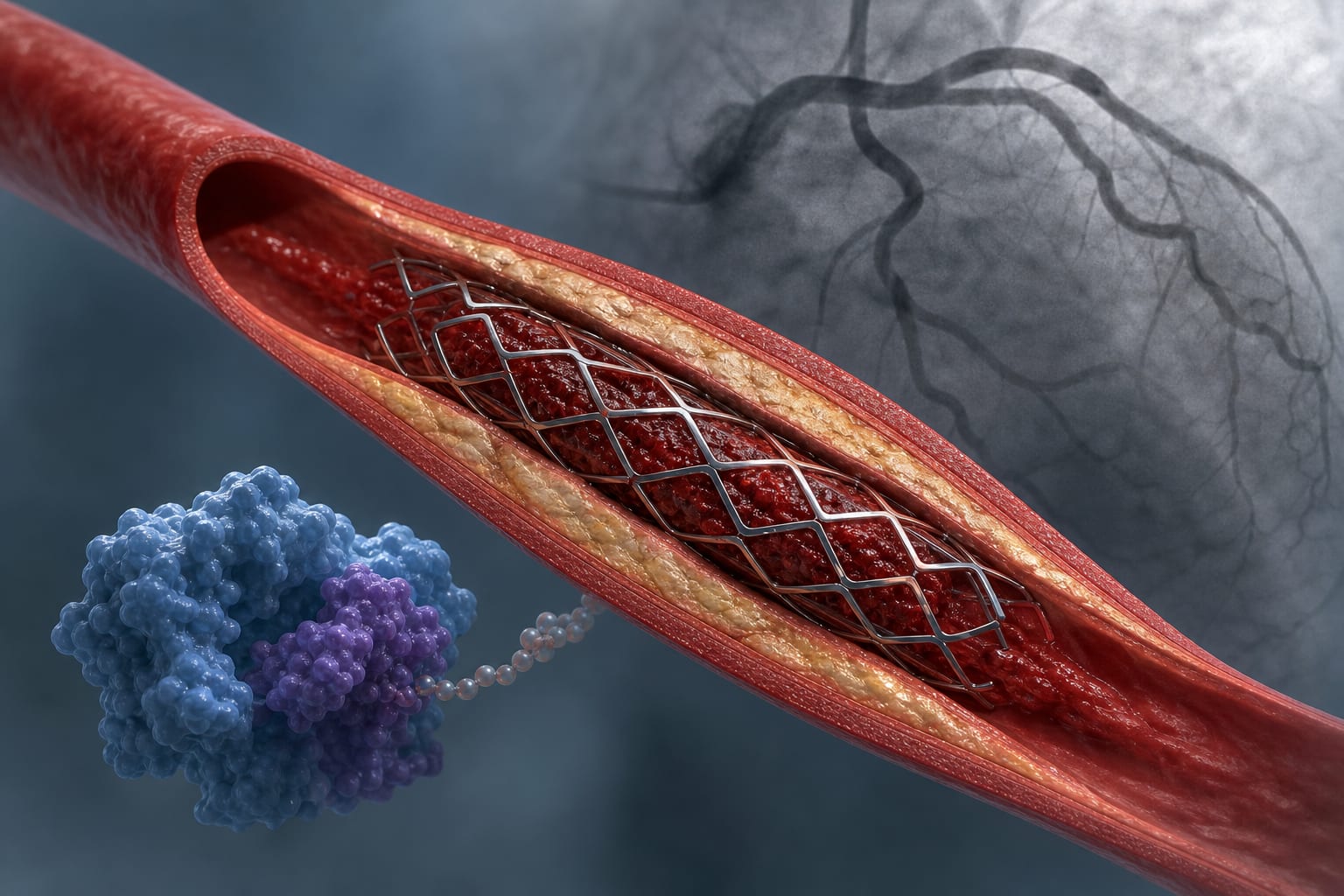
- Geometric correction is essential for effective catheter performance.
- A structured escalation strategy can restore functional access.
- Primary PCI was completed with a door-to-balloon time of 36 minutes.
- Correctability-focused approach enhances procedural success in tortuous anatomy.
Guideline-Based Recommendations
Diagnosis
- Electrocardiography to confirm ST-segment elevation in inferior leads.
Management
- Initiate dual antiplatelet therapy and anticoagulation in the emergency department.
Monitoring & Follow-up
- Continuous fluoroscopic guidance during catheter manipulation.
Risks
- Inadequate catheter support and ineffective torque transmission due to extreme tortuosity.
Patient & Prescribing Data
73-year-old woman with type 2 diabetes, hypertension, and coronary artery disease.
Loading doses of aspirin 300 mg and ticagrelor 180 mg were administered.
Clinical Best Practices
- Assess for bilateral radial artery patency prior to access.
- Utilize a correctability-oriented framework for managing arterial tortuosity.
- Consider sequential exchange to higher-support guidewires for effective loop straightening.
Related Resources & Content