Clinical Scorecard: Bilateral Corneal Flap Dislocation Without Trauma Two Decades Following LASIK Surgery
At a Glance
Category
Detail
Condition
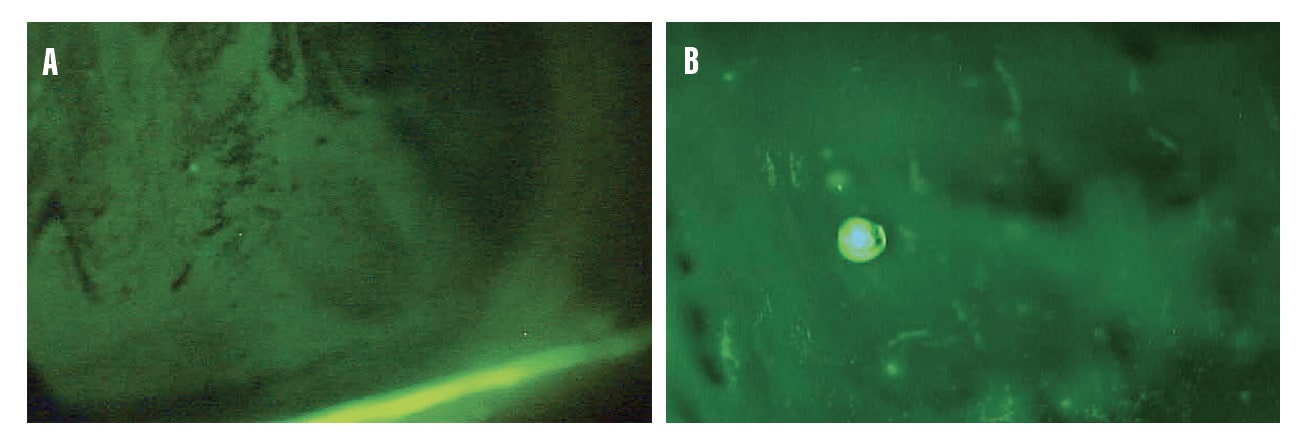
Late-onset bilateral corneal flap dislocation after LASIK without trauma
Key Mechanisms
Flap adhesion weakness, dry eye disease, eye rubbing, meibomian gland dysfunction leading to flap displacement
Target Population
Patients with history of LASIK surgery, especially with dry eye or MGD
Care Setting
Ophthalmology clinics and surgical centers
Key Highlights
Bilateral flap dislocation occurred 20 years post-LASIK without trauma, a rare presentation.
Severe dry eye and meibomian gland dysfunction contributed to flap instability and displacement.
Surgical flap repositioning with epithelial debridement and bandage lens placement led to symptom improvement.
Guideline-Based Recommendations
Diagnosis
Perform slit-lamp examination to assess corneal flap position, edema, wrinkling, and epithelial integrity.
Use anterior segment optical coherence tomography (AS-OCT) to confirm flap displacement and overlap.
Evaluate dry eye status including meibomian gland dysfunction signs and tear function tests (Schirmer I, TBUT).
Management
Prompt surgical intervention with flap lifting, epithelial cell debridement, stromal bed irrigation, and flap repositioning.
Use of bandage contact lenses postoperatively to protect the flap and promote healing.
Topical antibiotics and corticosteroids to control inflammation and prevent infection.
Address underlying dry eye and meibomian gland dysfunction with appropriate therapies.
Monitoring & Follow-up
Regular postoperative slit-lamp examinations to monitor flap attachment and detect epithelial ingrowth.
Corneal topography to assess corneal surface symmetry and stability after surgery.
Visual acuity assessments to evaluate functional recovery.
Risks
Flap dislocation risk persists even decades after LASIK, especially with dry eye and eye rubbing.
Potential for flap wrinkling, epithelial ingrowth, neovascularization, and vision loss if untreated.
Incomplete flap adhesion may predispose to recurrent displacement.
Patient & Prescribing Data
Patients with late-onset LASIK flap dislocation and dry eye disease
Combination of surgical flap repositioning and aggressive dry eye management improves outcomes; topical antibiotics and steroids are essential postoperatively.
Clinical Best Practices
Early recognition and surgical repair of flap dislocation to optimize visual recovery.
Comprehensive dry eye evaluation and treatment to reduce risk of flap displacement.
Careful intraoperative handling to remove epithelial debris and ensure flap centration.
Use of bandage lenses and anti-inflammatory medications post-surgery to support healing.
Dr. Theriot discusses the differences between natural tear film and artificial tears—and why the change in moniker to "lubricating drops" is appropriate.