Interferes with tear film dynamics, causing instability, reduced tear reservoir, obstruction of tear drainage, and promotes ocular surface inflammation.
Target Population
Individuals aged 60 years and older, affecting 44% to 98% of this demographic.
Care Setting
Ophthalmology clinics, particularly for diagnosis and management.
Key Highlights
CCh presents symptoms similar to dry eye disease (DED).
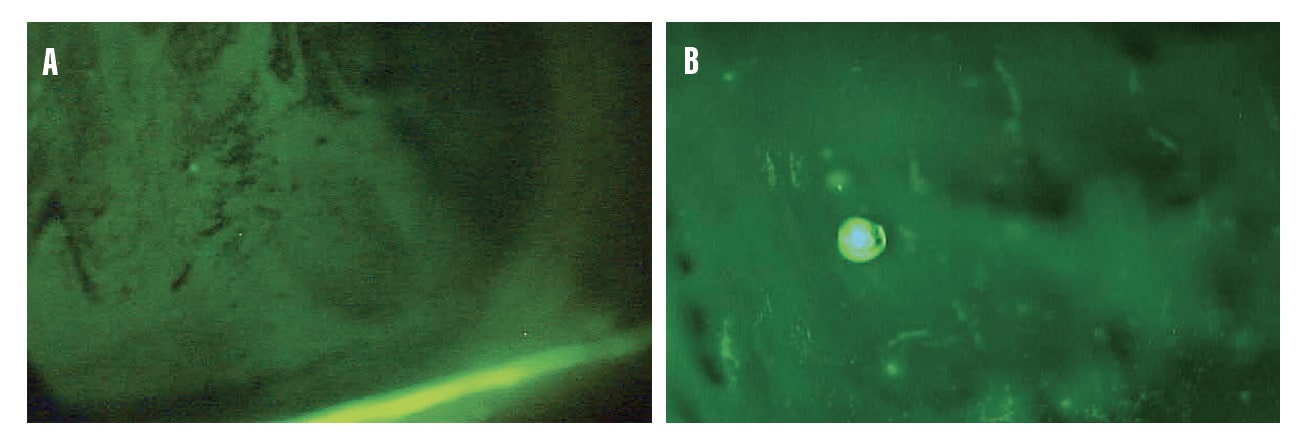
Diagnosis is primarily through slit lamp examination and vital dye application.
Initial treatment includes topical therapies; advanced cases may require surgical intervention.
CCh can worsen DED symptoms and is often unrecognized.
Practitioners should educate patients on CCh to improve understanding of persistent symptoms.
Guideline-Based Recommendations
Diagnosis
Use slit lamp examination to identify redundant conjunctival tissue.
Apply vital dyes to visualize folds and assess tear film.
Management
Initial treatments include topical steroids, immunomodulators, and preservative-free artificial tears.
Consider in-office procedures like plasma pen conjunctivoplasty for moderate to severe cases.
Monitoring & Follow-up
Assess symptom improvement and ocular surface condition regularly.
Risks
Untreated CCh can lead to chronic discomfort and worsening dry eye symptoms.
Patient & Prescribing Data
Older adults, particularly those with persistent dry eye symptoms.
Conservative medical therapy is the first step; surgical options may be necessary for severe cases.
Clinical Best Practices
Educate patients about the relationship between CCh and DED.
Perform thorough examinations to identify CCh in symptomatic patients.
Consider a multidisciplinary approach for managing complex cases.
Dr. Theriot discusses the differences between natural tear film and artificial tears—and why the change in moniker to "lubricating drops" is appropriate.