Clinical Scorecard: Practical Advantages of AI-Enhanced Fracture Identification in Pediatric Emergency Care
At a Glance
Category
Detail
Condition
Pediatric musculoskeletal fractures
Key Mechanisms
AI-supported software (RBFracture) using deep convolutional neural networks to detect fractures on radiographs as a second reader
Target Population
Children aged 2 to <18 years presenting with suspected fractures in emergency settings
Care Setting
Pediatric surgical emergency departments in tertiary care centers
Key Highlights
Musculoskeletal injuries are the most common reason for pediatric emergency admissions requiring radiographs.
Pediatric fractures have unique characteristics making diagnosis challenging, with potential severe long-term consequences if missed.
AI software RBFracture was evaluated for stand-alone performance and its impact on inexperienced physicians’ diagnostic accuracy in a real-life pediatric cohort.
Guideline-Based Recommendations
Diagnosis
Use pediatric radiologist assessment as the reference standard for fracture diagnosis.
Consider AI-assisted fracture detection as a complementary tool to improve diagnostic accuracy, especially for inexperienced readers.
Exclude radiographs of axial skeleton or skull and non-trauma cases from AI fracture detection use.
Management
Prompt and accurate diagnosis of pediatric fractures is critical to prevent long-term complications such as restricted joint mobility and impaired growth.
AI assistance should be integrated as a 'second pair of eyes' to support frontline physicians in emergency departments.
Monitoring & Follow-up
Monitor diagnostic confidence of physicians before and after AI assistance to assess impact on clinical decision-making.
Follow-up radiological and clinical assessments are essential to confirm fracture diagnosis and outcomes.
Risks
False negatives and false positives can occur when non-radiologists interpret pediatric radiographs without AI support.
AI models trained on adult fractures may not generalize well to pediatric fractures due to anatomical differences.
Diagnostic uncertainty should be resolved by consensus review or excluded if unresolved.
Patient & Prescribing Data
Pediatric patients aged 2 to <18 years undergoing emergency radiographic evaluation for suspected fractures.
AI software RBFracture can improve fracture detection accuracy and diagnostic confidence among inexperienced physicians, potentially reducing missed fractures and medicolegal risks.
Clinical Best Practices
Employ AI fracture detection software validated specifically for pediatric populations to complement human interpretation.
Ensure radiographs are evaluated by or reviewed with input from board-certified pediatric radiologists when possible.
Use a stepwise diagnostic approach: initial human assessment followed by AI-assisted reassessment without altering initial findings.
Consider questionable AI findings conservatively as fractures to minimize missed diagnoses.
Exclude cases with persistent diagnostic uncertainty from clinical decision-making or seek consensus review.
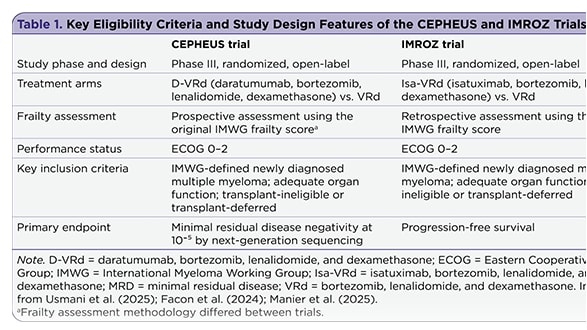
The management of newly diagnosed transplant-ineligible multiple myeloma remains challenging, in part due to the complexity of treatment decisions for frail patients. Recent subgroup analyses provide insight into whether quadruplet therapy may offer advantages over triplet therapy in this population.