Sphincter-saving surgery versus abdominoperineal resection in low rectal cancer: the role of indocyanine green fluorescence angiography in surgical decision-making - Scorecard - MDSpire
Advertisement
Sphincter-saving surgery versus abdominoperineal resection in low rectal cancer: the role of indocyanine green fluorescence angiography in surgical decision-making
Clinical Scorecard: Comparing Sphincter-Sparing Surgery and Abdominoperineal Resection for Low Rectal Cancer: The Impact of Indocyanine Green Fluorescence Angiography on Surgical Choices
At a Glance
Category
Detail
Condition
Low Rectal Cancer
Key Mechanisms
Indocyanine green fluorescence angiography (ICG-FA) assesses bowel perfusion to prevent anastomotic failure.
Target Population
Patients with low rectal cancer (≤6 cm from the anal verge).
Care Setting
Tertiary academic surgical department.
Key Highlights
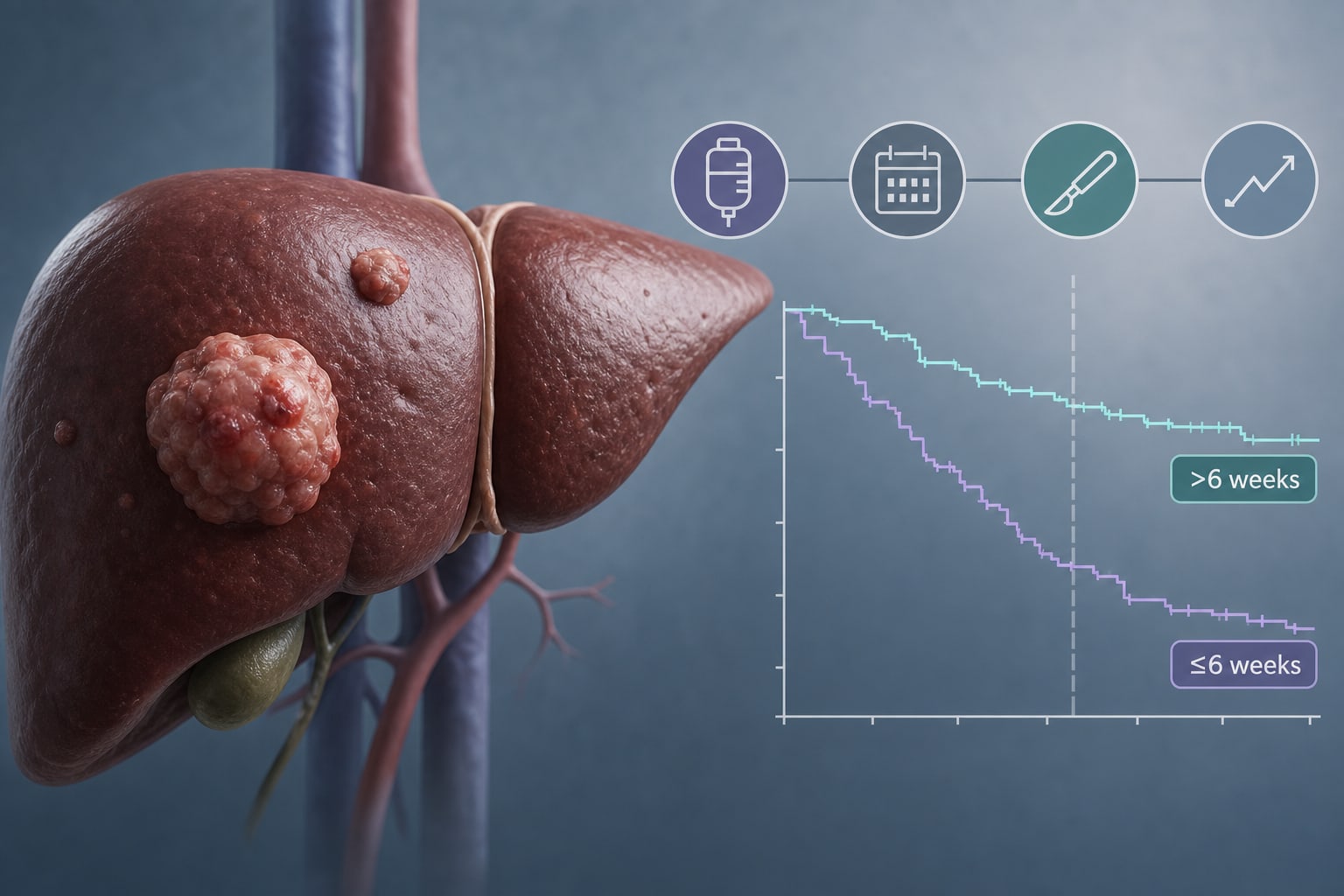
ICG-FA modified the resection line in 40% of patients assessed.
Radical (R0) resection achieved in 19 of 21 patients with margin status recorded.
Postoperative complications occurred in 56% of patients, mostly Clavien–Dindo grade I–II.
No 30-day mortality reported; one late in-hospital death occurred beyond 30 days.
Sphincter-saving surgery is feasible but carries substantial morbidity.
Guideline-Based Recommendations
Diagnosis
Histologically proven colorectal adenocarcinoma.
Management
Consider sphincter-saving surgery versus abdominoperineal resection based on tumor characteristics and patient factors.
Monitoring & Follow-up
Postoperative assessment for complications, particularly anastomotic leaks.
Risks
Inadequate perfusion of the proximal colonic stump is a leading cause of anastomotic failure.
Patient & Prescribing Data
Patients undergoing surgery for low rectal cancer.
ICG-FA is a low-risk adjunct that informs intraoperative decision-making.
Clinical Best Practices
Utilize ICG-FA in all sphincter-saving procedures for low rectal cancer.
Integrate tumor-related and patient-related variables in surgical decision-making.