Clinical Scorecard: Screening for Diabetic Retinopathy in a Rural High-Latitude Community in Northern Norway
At a Glance
Category
Detail
Condition
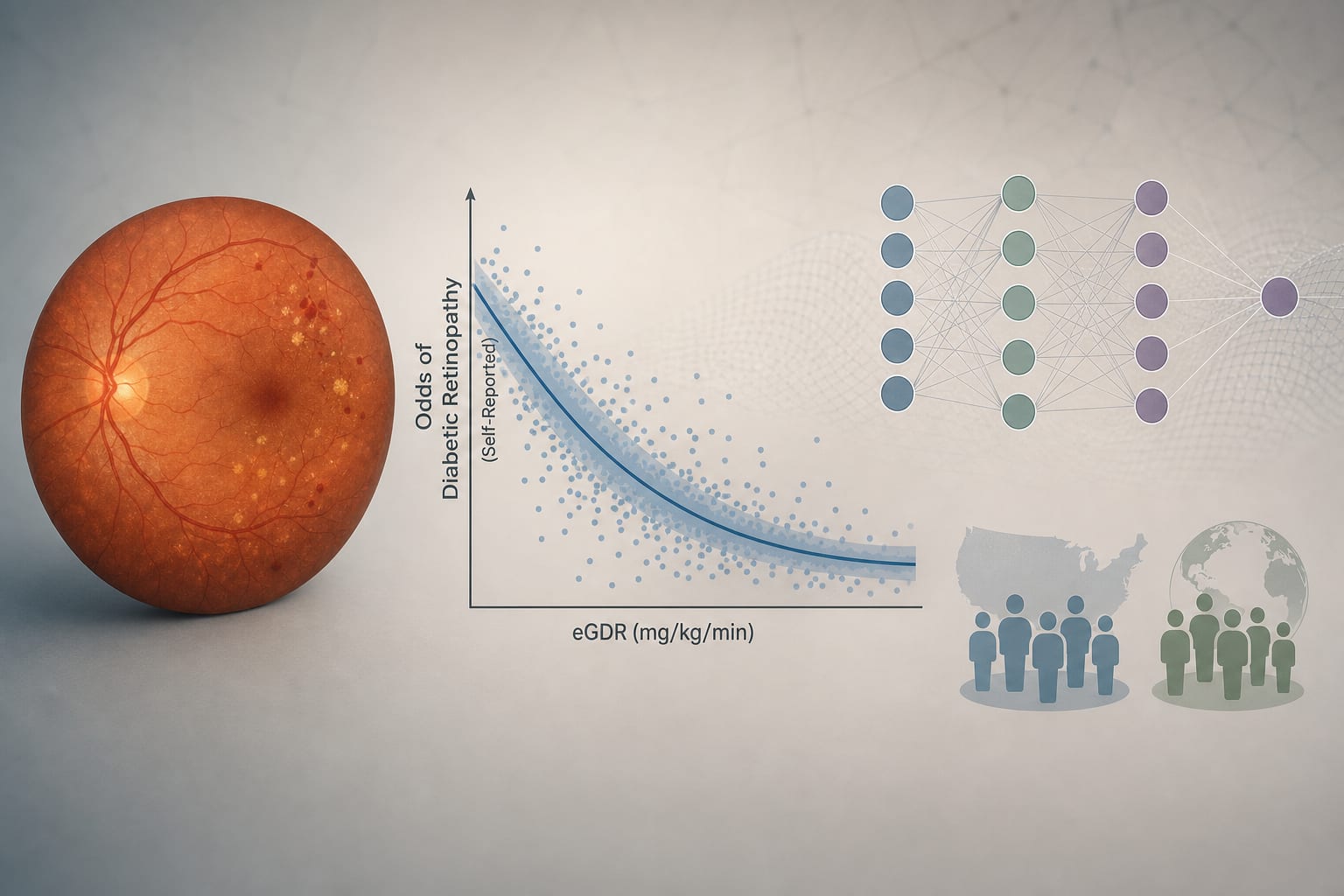
Diabetic retinopathy (DR), a neurovascular complication of diabetes causing vision impairment and blindness
Key Mechanisms
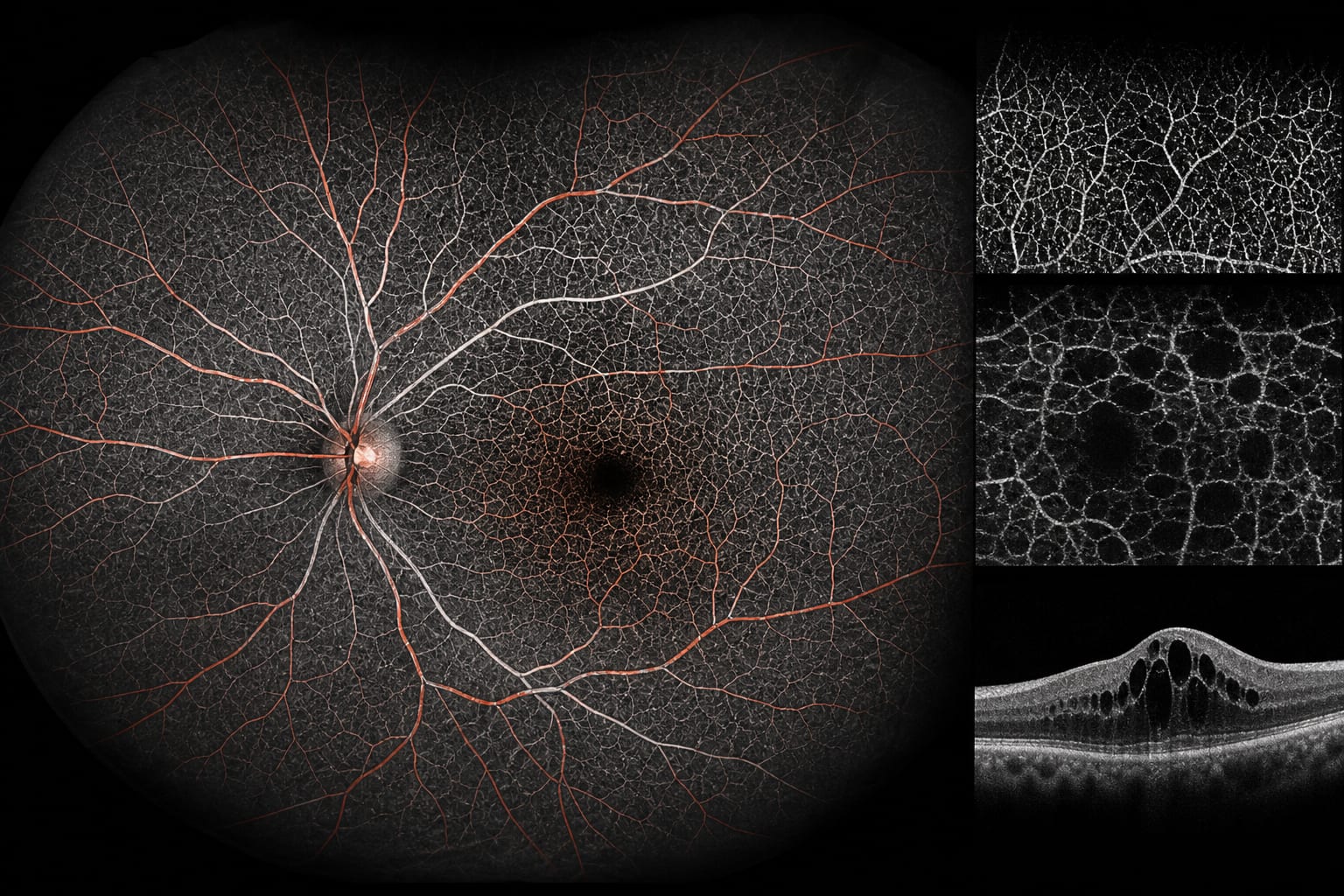
Retinal neurovascular damage progressing from no DR to proliferative DR and diabetic macular edema (DME), detectable by retinal imaging and OCT
Target Population
Adults aged ≥18 years with diabetes attending routine diabetic retinal screening in rural northern Norway
Care Setting
Outpatient eye clinic in a rural hospital serving a geographically dispersed population
Key Highlights
DR prevalence globally is approximately 22.27%, with vision-threatening DR at 6.17%; prevalence varies widely by region.
Norwegian guidelines recommend a two-step screening model with primary grading by certified nurses/optometrists and secondary grading by ophthalmologists for moderate or worse DR.
This study evaluates the safety and quality of the two-step screening model implemented in Finnmark, a rural northern Norwegian region with high diabetes prevalence.
Guideline-Based Recommendations
Diagnosis
Use retinal photography for initial DR screening; optical coherence tomography (OCT) is not included in the screening protocol per Norwegian guidelines.
Grade DR severity according to the International Clinical Disease Severity Scale: no DR, mild NPDR, moderate NPDR, severe NPDR, proliferative DR.
Define diabetic macular edema (DME) based on retinal photography and OCT findings, distinguishing clinically significant and non-clinically significant DME.
Management
Refer images indicating moderate or more severe DR to ophthalmologists for secondary grading.
Implement a two-step screening model to optimize resource use and reduce ophthalmologist workload.
Monitoring & Follow-up
Perform regular retinal screening to detect early DR changes, as early stages often lack symptoms.
Assess image quality rigorously to ensure gradability and accurate diagnosis.
Use a worst-eye approach for participant-level DR grading.
Risks
Task-shifting to non-ophthalmologist graders may increase risk of missed sight-threatening disease or unnecessary referrals.
Accept HbA1c values up to 12 months old due to limited access to primary care records, though guidelines recommend within 6 months.
Patient & Prescribing Data
Patients with diabetes aged 18 years and older undergoing routine retinal screening in a rural high-latitude community.
Early detection through systematic screening enables timely intervention to reduce visual impairment and associated costs.
Clinical Best Practices
Use certified nurses or optometrists for primary grading of retinal images to optimize ophthalmologist workload.
Ensure mydriasis before retinal imaging to improve image quality.
Employ standardized grading scales and criteria for DR and DME to maintain consistency.
Mask graders to each other’s assessments and use a retina specialist for adjudication when consensus is lacking.
Collect and document HbA1c values within 12 months to support clinical assessment.
Analysis of more than 61,000 patients found higher odds of elevated loneliness scores among those reporting blindness and those with diabetic retinopathy, but not among patients with glaucoma or age-related macular degeneration.