Clinical Scorecard: Uncommon Presentation of Ocular Giant Cell Arteritis: Bilateral Orbital Inflammation and Diagnostic Difficulties
At a Glance
Category
Detail
Condition
Key Mechanisms
Target Population
Individuals over the age of 50, particularly those with risk factors such as hypertension, with a higher incidence in women and Northern European populations.
Care Setting
Key Highlights
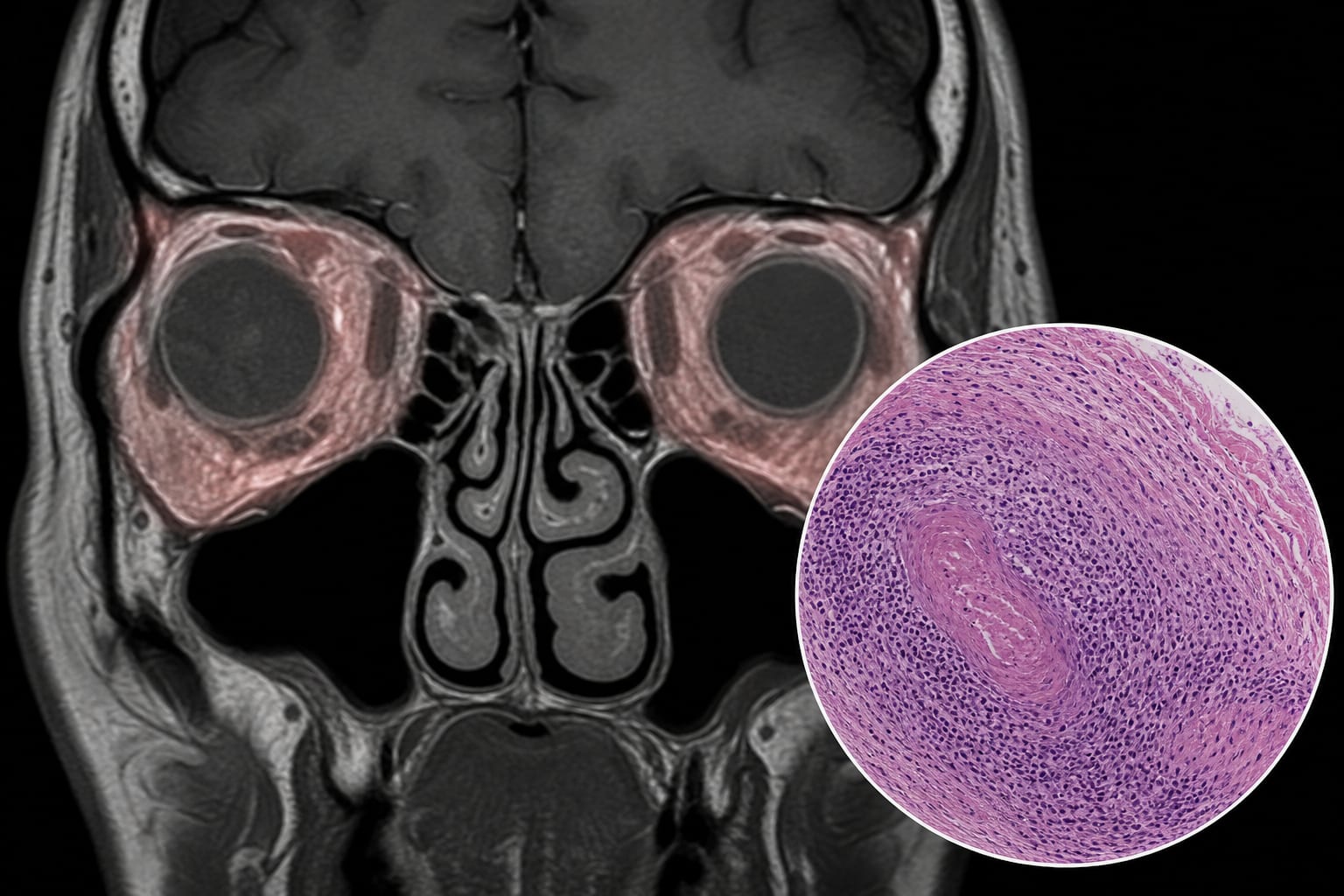
GCA can present with atypical ocular symptoms, including bilateral orbital inflammation.
Diagnostic challenges exist due to normal inflammatory markers in some cases.
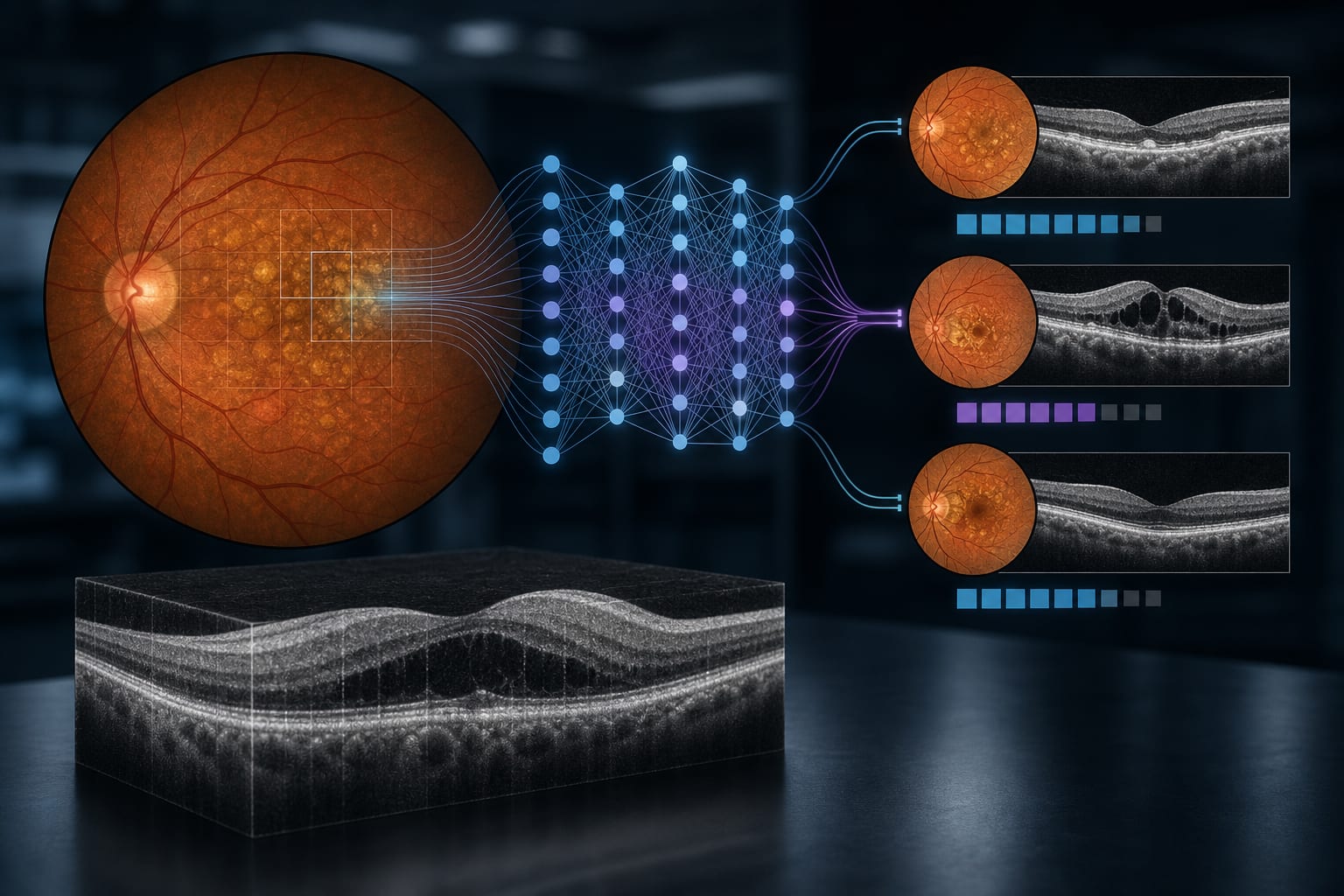
High-resolution MRI can reveal critical findings such as optic nerve sheath enhancement.
Temporal artery biopsy remains the confirmatory standard for diagnosis.
Corticosteroid use can lead to significant morbidity, highlighting the need for steroid-sparing agents.
Recognizing atypical presentations is crucial for timely diagnosis and management.
Guideline-Based Recommendations
Diagnosis
Utilize the 2022 ACR/EULAR classification criteria, incorporating advanced imaging modalities.
Consider high-resolution MRI for detecting vessel wall inflammation.
Management
Initiate high-dose intravenous steroids for acute management.
Consider steroid-sparing agents like Tocilizumab and JAK inhibitors.
Monitoring & Follow-up
Regular follow-up for vision changes and complications from steroid use.
Risks
Potential for visual loss if GCA is not promptly diagnosed and treated.
Patient & Prescribing Data
High-dose IV steroids can lead to initial improvement, but long-term management may require tapering, alternative therapies, and monitoring for complications from steroid use.
Clinical Best Practices
Be vigilant for atypical presentations of GCA, especially in older patients.
Incorporate neuroimaging in cases with suspected ocular involvement.
Monitor inflammatory markers, but be aware of their limitations.
Consider neuroimaging for atypical presentations to aid in diagnosis.