Impact of kimura-takemoto atrophy classification on first-line H. pylori eradication: a retrospective cohort study
-
By
-
Dongchu Wang
-
Xiangwu Ding
-
Aixiang Wang
-
June 19, 2026
-
Clinical Scorecard: Influence of Kimura-Takemoto Atrophy Staging on the Success of Initial H. pylori Eradication: A Retrospective Cohort Analysis
At a Glance
| Category | Detail |
|---|
| Condition | Chronic Atrophic Gastritis |
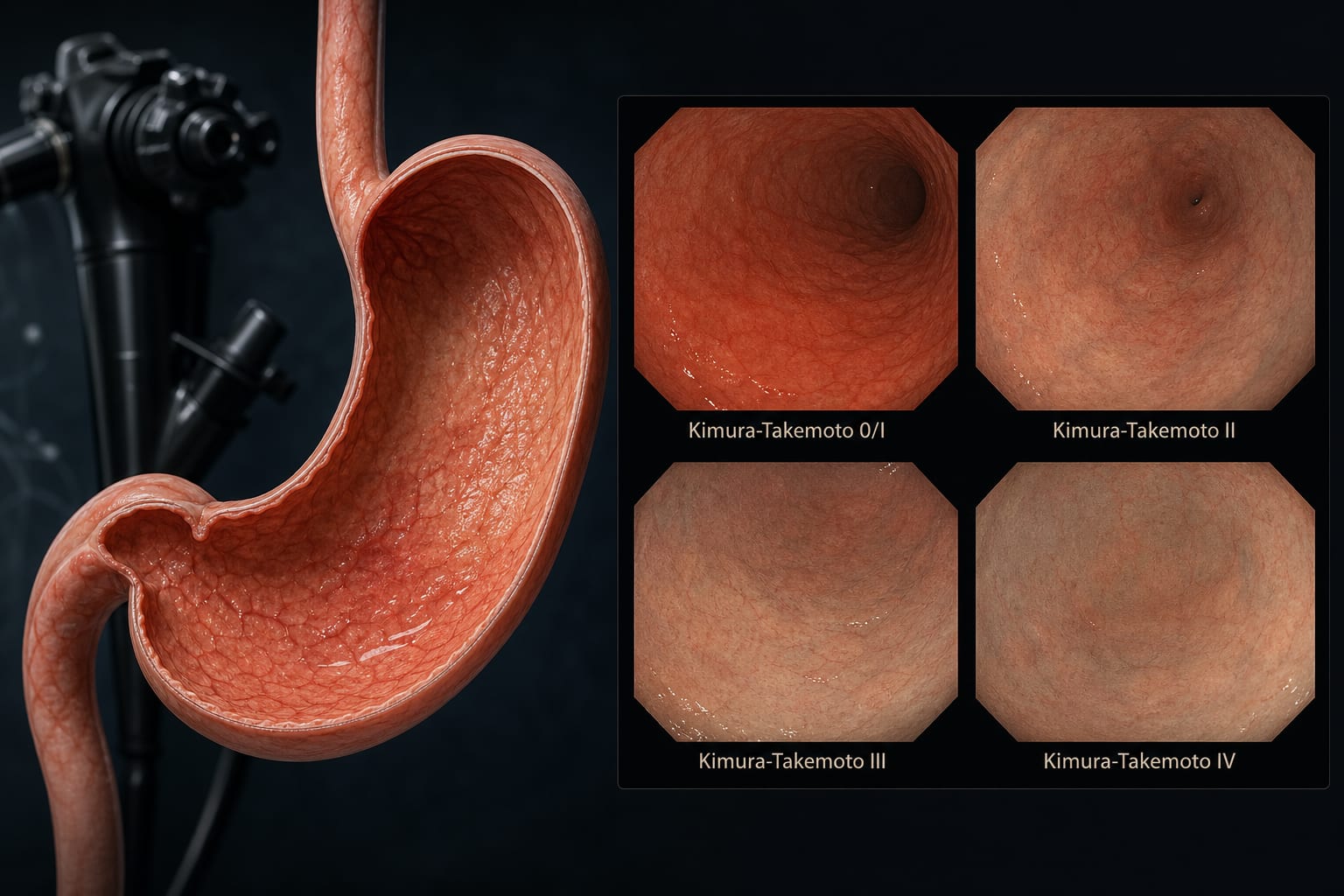
| Key Mechanisms | Endoscopic grading of gastric atrophy using the Kimura-Takemoto classification impacts H. pylori eradication success. |
| Target Population | Patients aged 18–85 with chronic atrophic gastritis and H. pylori infection. |
| Care Setting | Single-center retrospective cohort study. |
Key Highlights
- Overall H. pylori eradication rate was 76.6%.
- Eradication rate in open-type atrophy group was 42.3%.
- Closed-type atrophy group had an eradication rate of 83.6%.
- Open-type atrophy was independently associated with eradication failure (OR = 8.287).
- Alternative regimens are recommended for patients with open-type atrophy.
Guideline-Based Recommendations
Diagnosis
- Confirm H. pylori infection via urea breath test.
- Assess gastric atrophy using high-definition white-light gastroscopy.
Management
- Use bismuth-containing quadruple regimen as first-line therapy.
- Consider clarithromycin-free regimens for open-type atrophy.
Monitoring & Follow-up
- Follow-up with urea breath test at least 4 weeks post-treatment.
Risks
- Increased risk of eradication failure in patients with open-type gastric atrophy.
Patient & Prescribing Data
Patients diagnosed with chronic atrophic gastritis and H. pylori infection.
Bismuth-containing quadruple therapy is standard; alternative regimens may be necessary for open-type atrophy.
Clinical Best Practices
- Utilize the Kimura-Takemoto classification for assessing gastric atrophy.
- Individualize treatment based on the type of gastric atrophy.
Related Resources & Content