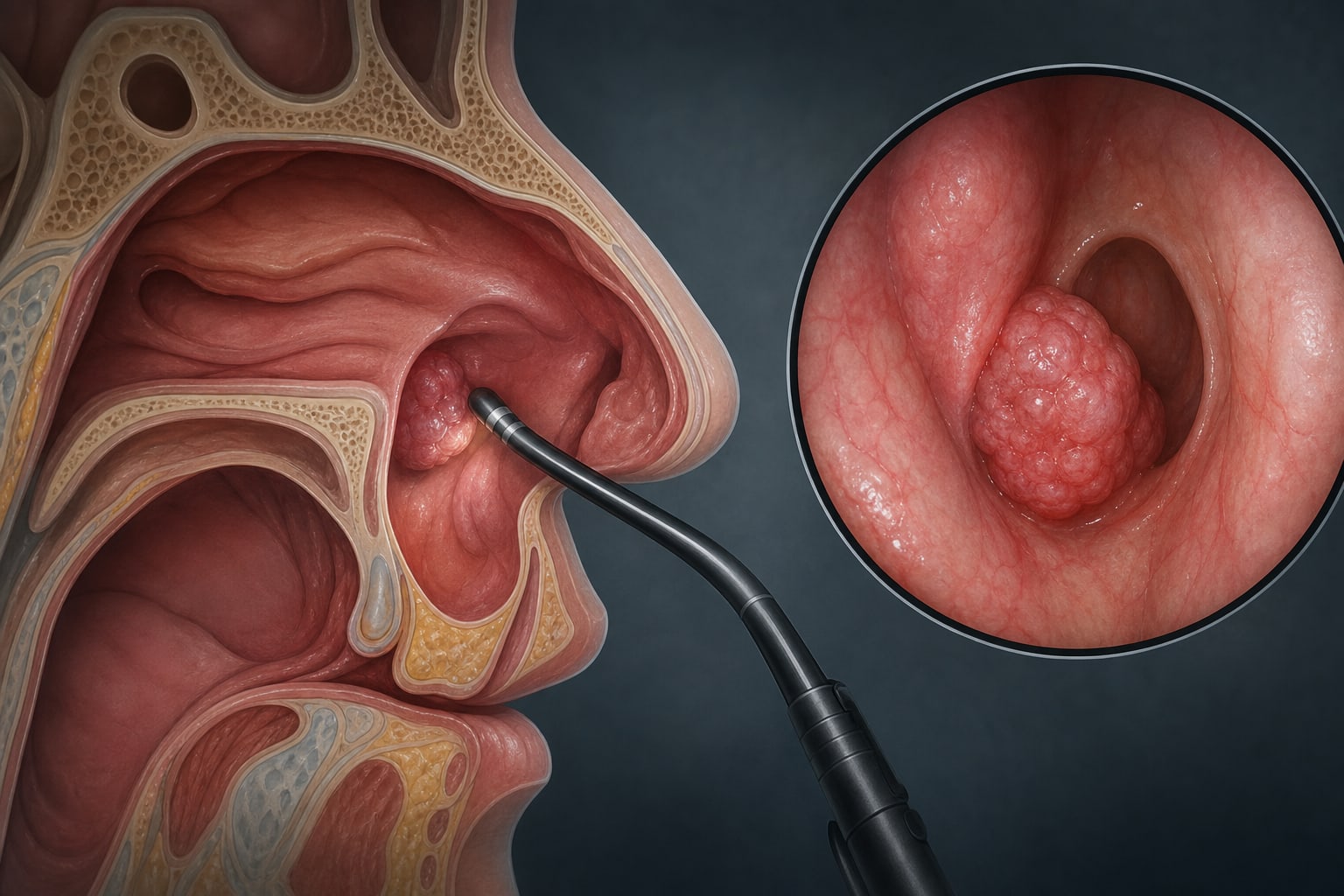
Reactive lymphoid hyperplasia of the eustachian tube orifice presenting with aural fullness: a case report
By
Lingping Ding
Qi Wu
Zhaoli Meng
June 25, 2026
Clinical Scorecard: Case Report: Aural Fullness Due to Reactive Lymphoid Hyperplasia at the Eustachian Tube Orifice
At a Glance
Category Detail
Condition Reactive Lymphoid Hyperplasia Key Mechanisms Benign immune-mediated response to chronic inflammation or stimulation. Target Population Adults presenting with aural fullness and hearing loss. Care Setting Clinical evaluation and surgical management of lesions at the eustachian tube orifice.
Key Highlights
Rare occurrence of benign lymphoid hyperplasia at the eustachian tube orifice. Initial misdiagnosis as otitis media with effusion due to overlapping symptoms. Histopathological confirmation of benign lymphoid hyperplasia post-surgery. Significant improvement in symptoms following navigated endoscopic resection. Importance of comprehensive evaluation to avoid misdiagnosis. Guideline-Based Recommendations
Diagnosis
Histopathology and immunohistochemistry are essential for definitive diagnosis. Management
Navigated endoscopic resection is recommended for symptomatic lesions. Monitoring & Follow-up
Follow-up with endoscopy and MRI if new clinical complaints arise. Risks
Risk of misdiagnosis leading to overtreatment of benign lesions. Patient & Prescribing Data
58-year-old male with persistent aural fullness and hearing loss.
Postoperative improvement in symptoms with complete resolution of aural fullness and tinnitus.
Clinical Best Practices
Consider differential diagnosis for eustachian tube dysfunction symptoms. Utilize imaging and endoscopic evaluation for suspected lesions. Ensure histopathological confirmation before concluding malignancy. Related Resources & Content