Patients with heart failure, especially those with reduced ejection fraction
Care Setting
Cardiovascular rehabilitation and preventive cardiology settings
Key Highlights
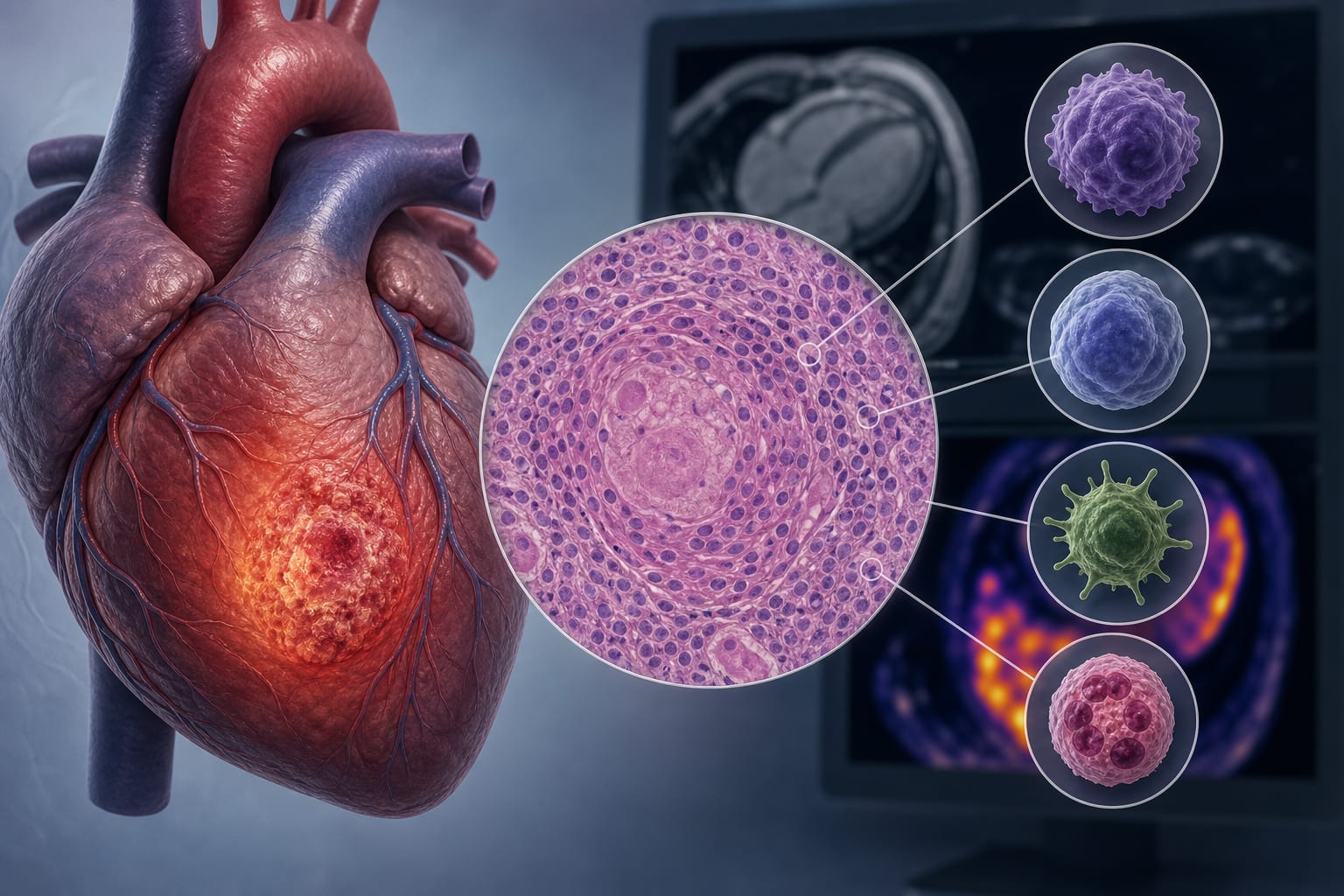
Structured physical training significantly reduces circulating proinflammatory cytokines IL-6 and TNF-α in heart failure patients
Reductions in IL-6 and TNF-α correlate with improvements in maximal oxygen consumption (VO₂ max) and left ventricular ejection fraction, indicating a dose–response relationship
Exerkines serve as dynamic biomarkers reflecting biological adaptations and may guide personalized exercise prescriptions and monitoring
Guideline-Based Recommendations
Diagnosis
Consider measuring circulating proinflammatory cytokines (IL-6, TNF-α) as biomarkers to assess inflammatory status in heart failure
Management
Implement structured physical exercise programs to reduce systemic inflammation and improve cardiac and skeletal muscle function
Tailor exercise prescriptions based on functional and molecular responses to optimize rehabilitation outcomes
Monitoring & Follow-up
Use exerkine levels alongside traditional functional metrics (e.g., VO₂ max, ejection fraction) to monitor patient response and compliance during rehabilitation
Risks
Further research needed to determine optimal exercise intensity and volume to maximize benefits and ensure safety, especially in advanced heart failure
Patient & Prescribing Data
Patients with heart failure enrolled in structured physical training programs
Exercise reduces proinflammatory cytokines IL-6 and TNF-α, correlating with improved cardiac function and exercise capacity; effects stronger in reduced ejection fraction
Clinical Best Practices
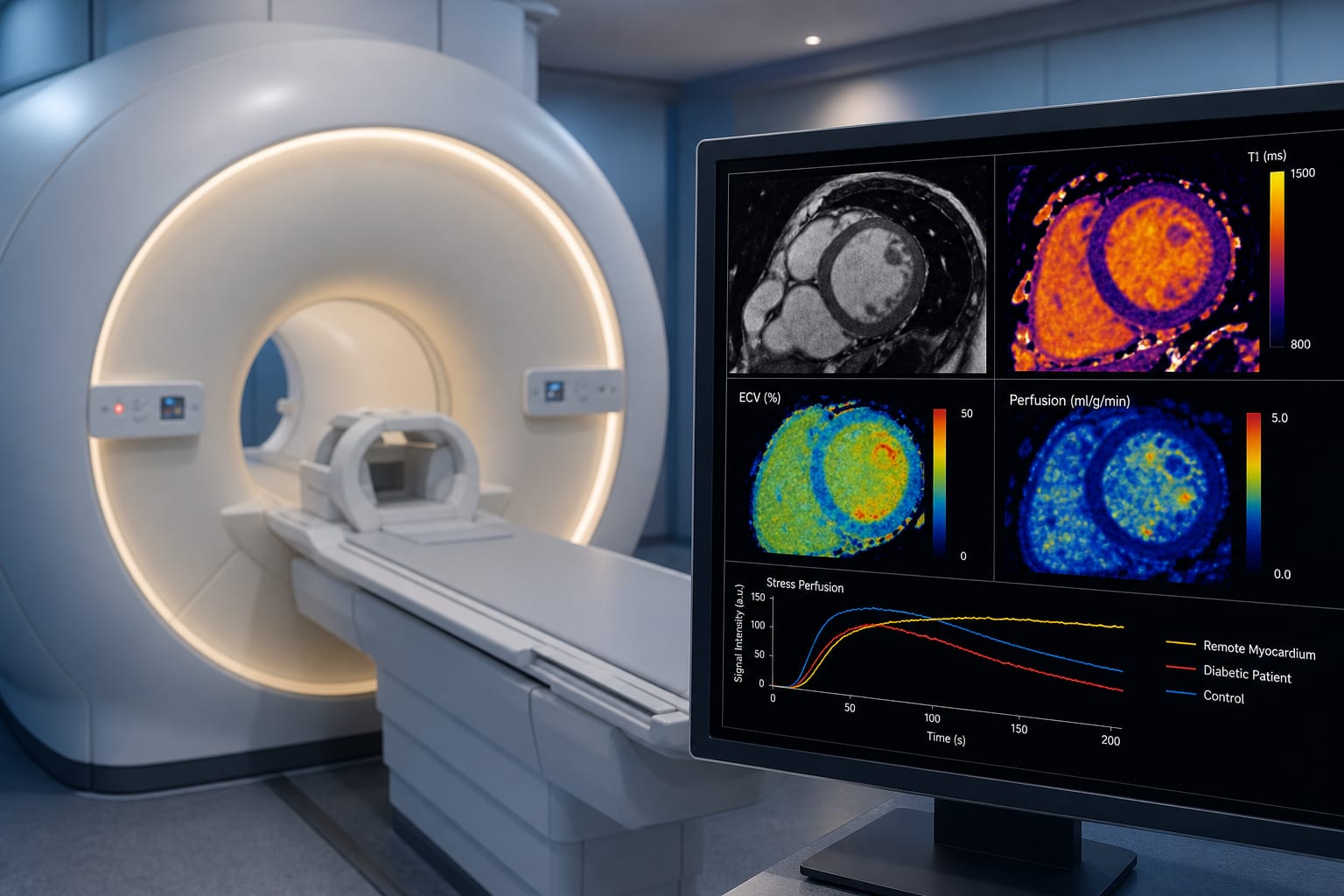
Incorporate biomarker profiling (exerkines) with cardiopulmonary exercise testing and imaging for comprehensive patient assessment
Personalize exercise interventions considering molecular responses and patient-specific factors
Address psychosocial and behavioral aspects to promote sustained physical activity adherence
Recognize exercise as a modulator of inflammatory and metabolic pathways influencing heart failure progression