Clinical Scorecard: Knee OA Pain: Inulin vs Physiotherapy Effects
At a Glance
Category
Detail
Condition
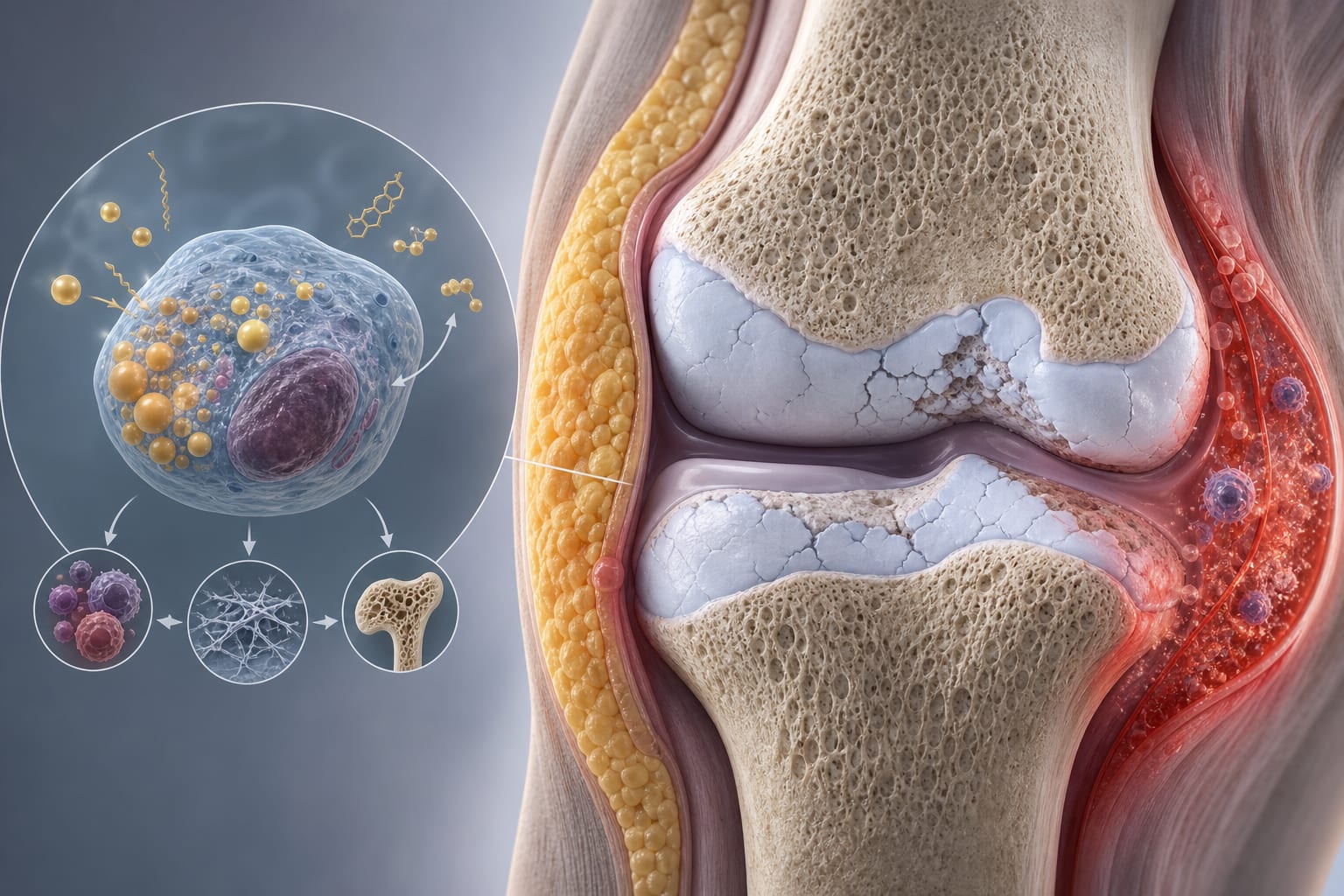
Knee osteoarthritis (OA)
Key Mechanisms
Inulin increases circulating butyrate and GLP-1, improving proximal and central sensitization; physiotherapy-supported exercise improves physical function
Target Population
Community-dwelling patients with knee osteoarthritis
Care Setting
Outpatient/community care
Key Highlights
Both inulin supplementation and physiotherapy-supported exercise reduced knee OA pain over 6 weeks, each exceeding the minimum clinically important difference on the Numerical Rating Scale.
Physiotherapy improved physical function (sit-to-stand and timed up-and-go tests), while inulin improved grip strength and increased pressure pain thresholds.
No synergistic pain reduction was observed when combining inulin with physiotherapy; dropout rates were lower with inulin than physiotherapy.
Guideline-Based Recommendations
Diagnosis
Use Numerical Rating Scale to assess baseline and changes in knee OA pain.
Management
Consider inulin supplementation as a dietary intervention to reduce pain and improve grip strength in knee OA patients.
Implement physiotherapy-supported exercise programs to reduce pain and improve physical function.
Combined use of inulin and physiotherapy does not provide additional synergistic pain relief.
Monitoring & Follow-up
Monitor pain changes using Numerical Rating Scale.
Assess physical function improvements via sit-to-stand and timed up-and-go tests.
Observe for minor gastrointestinal adverse events with inulin supplementation.
Risks
Minor gastrointestinal adverse events may occur with inulin but do not typically lead to treatment discontinuation.
Higher dropout rates observed in physiotherapy-supported exercise groups.
Patient & Prescribing Data
Community-dwelling adults with knee osteoarthritis
Inulin is well tolerated with low dropout rates and improves pain and grip strength; physiotherapy improves pain and functional mobility but has higher dropout rates.
Clinical Best Practices
Use a 6-week intervention period to evaluate pain and functional outcomes.
Adjust analyses for baseline values and consider intention-to-treat approaches with imputation for missing data.
Educate patients on potential minor gastrointestinal effects of inulin to improve adherence.
Recognize that physiotherapy requires patient engagement and may have higher dropout rates.
Consider integrating dietary interventions like inulin alongside physiotherapy for a holistic approach to knee OA management.