Clinical Scorecard: In Vivo 9.4 Tesla MRI Imaging in a Patient with Drug-Resistant Epilepsy: A Technical Overview
At a Glance
Category
Detail
Condition
Drug-Resistant Epilepsy (DRE)
Key Mechanisms
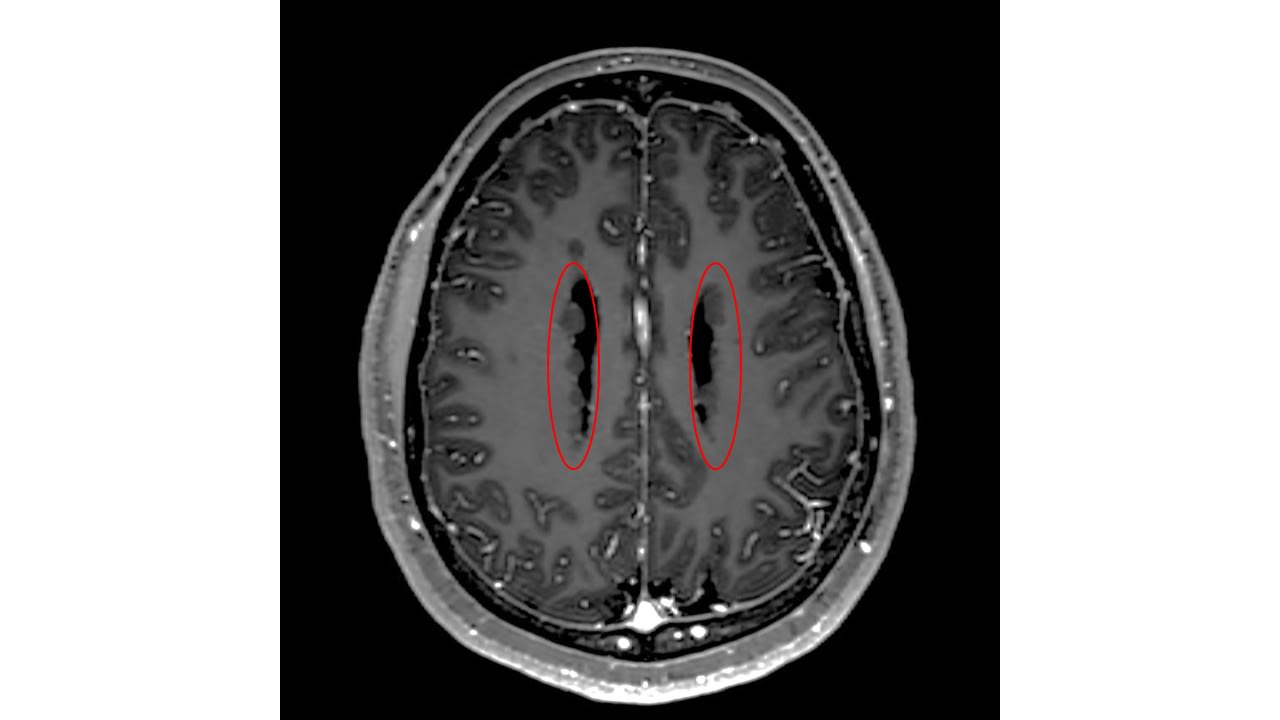
Ultra-high field MRI (9.4T) improves detection and delineation of epileptogenic lesions by increasing spatial resolution and contrast-to-noise ratio, aiding pre-surgical localization.
Target Population
Patients with focal drug-resistant epilepsy, especially those MRI-negative at 3T and 7T
Care Setting
Specialized epilepsy centers with access to ultra-high field MRI research facilities
Key Highlights
Approximately 30–40% of focal epilepsy patients have drug-resistant epilepsy; 30% of these are MRI-negative at 3T.
Ultra-high field MRI at 7T and 9.4T improves lesion detection rates, with 7T showing up to 30% increase over 3T.
9.4T MRI requires parallel transmit technology to mitigate B1+ inhomogeneities and careful SAR management.
Guideline-Based Recommendations
Diagnosis
Use dedicated epilepsy MRI protocols with expert neuroradiologist assessment to maximize lesion detection.
Consider ultra-high field MRI (7T or 9.4T) for patients with drug-resistant epilepsy who are MRI-negative at 3T.
Apply parallel transmit (pTx) technology at 9.4T to address RF field inhomogeneities.
Management
Use improved lesion detection from UHF MRI to guide surgical candidacy and planning for epilepsy surgery.
Balance MRI sequence design to optimize signal-to-noise ratio and contrast while minimizing specific absorption rate.
Monitoring & Follow-up
Monitor patient tolerance during ultra-high field MRI scanning for transient symptoms such as dizziness.
Perform independent image quality and lesion assessment by experienced neuroradiologists and epilepsy surgeons.
Risks
Increased magnetic field inhomogeneities and RF power deposition at 9.4T require technical mitigation.
Potential transient dizziness during patient positioning in the MRI bore.
Patient & Prescribing Data
Adult patients with drug-resistant focal epilepsy and negative findings on conventional 3T and 7T MRI
9.4T MRI provides higher spatial resolution (0.6 mm cubic) and improved visualization of epileptogenic structures, potentially enabling surgical intervention in previously MRI-negative cases.
Clinical Best Practices
Employ a dedicated epilepsy MRI protocol tailored for ultra-high field imaging.
Use parallel transmit coils and universal pTx pulses to manage B1+ inhomogeneities at 9.4T.
Involve multidisciplinary teams including neuroradiologists experienced in epilepsy imaging and epilepsy surgeons for image interpretation.
Ensure patient informed consent and monitor for adverse effects during UHF MRI scanning.
Compare imaging findings across 3T, 7T, and 9.4T to assess incremental diagnostic value.
by Rick H. G. J. van Lanen, Daniel Uher, Desmond H. Y. Tse, Esther Steijvers, Albert J. Colon, Jacobus F. A. Jansen, Gerhard S. Drenthen, Dimo Ivanov, Govert Hoogland, Kim Rijkers, Christianne M. Hoeberigs, Paul A. M. Hofman, Walter H. Backes, Olaf E. M. G. Schijns
Aviva Abosch, M.D., Ph.D., a neurosurgeon at Baptist Health Miami Neuroscience Institute, part of Baptist Health Brain and Spine Care, was installed as the Esernia Endowed Chair in Surgical Treatment of Adult Epilepsy and Movement Disorders.
Epilepsy remains a life-altering condition, particularly due to the unpredictable nature of seizures and their cumulative impact on cognition, independence and quality of life.