Clinical Scorecard: Revisional Surgery Using Single-Anastomosis Sleeve Jejunal (SAS-J) Bypass Following Initial Restrictive Bariatric Interventions
At a Glance
Category
Detail
Condition
Morbid obesity with weight regain or failure after primary restrictive bariatric procedures
Key Mechanisms
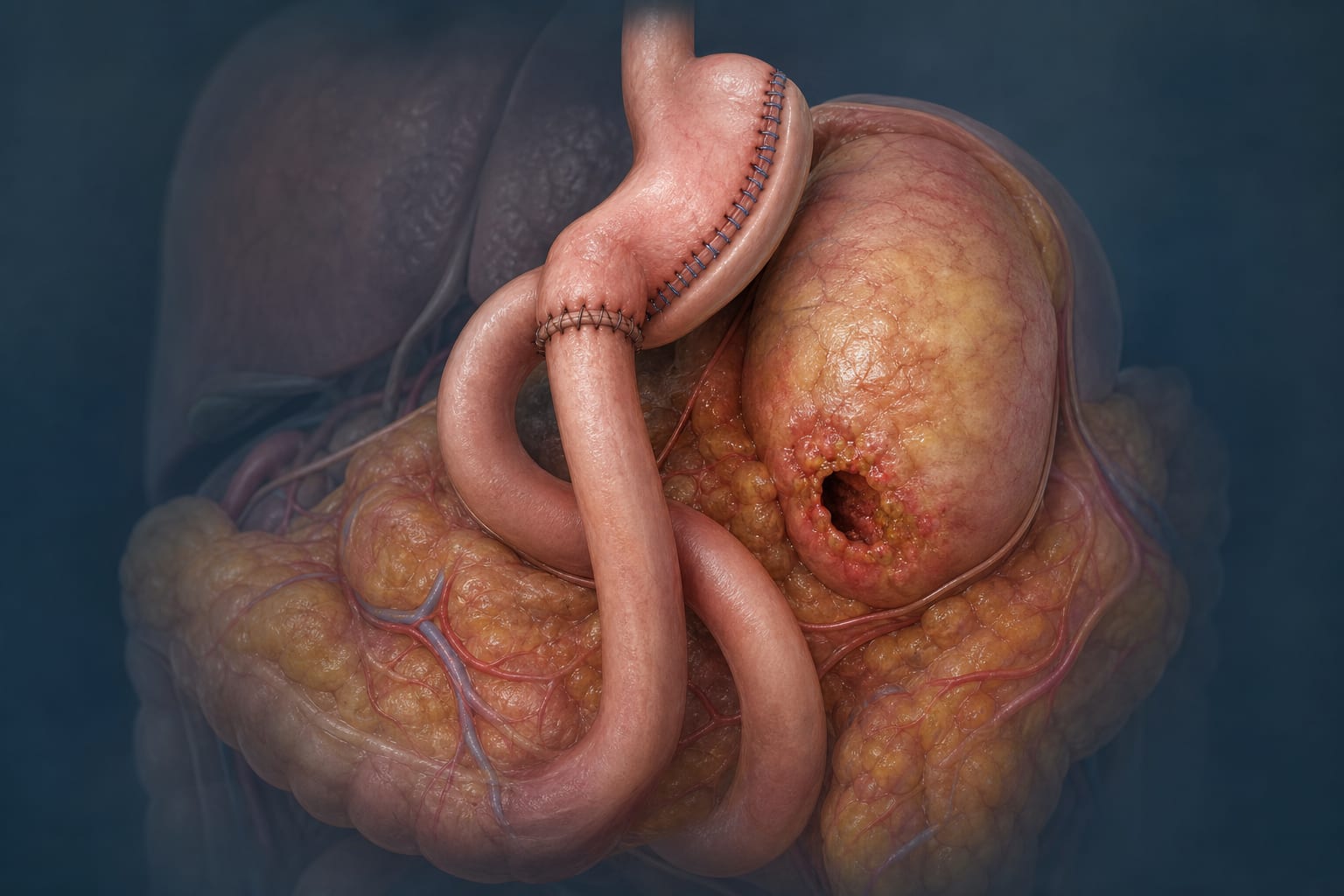
SAS-J bypass combines sleeve gastrectomy with a single-anastomosis jejunal bypass to induce weight loss via restriction and mild malabsorption
Target Population
Patients with weight regain or failure after initial restrictive bariatric surgeries such as LSG, LAGB, or gastric plication
Care Setting
Specialized bariatric surgical centers with experienced surgeons
Key Highlights
Weight regain after restrictive bariatric procedures is common, with failure rates up to 30–60%.
SAS-J bypass offers a revisional surgical option with advantages including relative simplicity, less malnutrition, and easy upper GI tract screening.
Standardized surgical technique involves sleeve creation and jejunal anastomosis at one-third of total small bowel length from the duodenojejunal junction.
Guideline-Based Recommendations
Diagnosis
Define failure as EWL < 50%, BMI ≥ 35 kg/m2, or unsatisfactory control of obesity-related comorbidities.
Define weight regain as BMI increase to > 35 kg/m2 after initial successful weight loss.
Perform routine CT gastric volumetry and upper GI endoscopy in symptomatic or band cases before revisional surgery.
Management
Consider SAS-J bypass as a revisional procedure after failure or weight regain following restrictive bariatric surgeries.
Ensure psychological consultation and patient consent emphasizing lifestyle modification as essential for long-term success.
Perform revisional surgery at least 5 years after primary operation with prior nutritional counseling.
Monitoring & Follow-up
Monitor for postoperative complications given higher risk compared to primary procedures.
Follow up on weight loss outcomes and comorbidity control post-revisional surgery.
Assess for signs of gastric torsion or emptying disorders due to prior ligament division.
Risks
Higher complication rates and longer hospital stay compared to primary bariatric surgeries.
Potential for gastric volvulus or twisting if stomach fixation is inadequate.
Weight regain risk if patient noncompliance with lifestyle changes persists.
Patient & Prescribing Data
Patients with prior restrictive bariatric surgery experiencing weight regain or failure
SAS-J bypass is effective as a revisional procedure with advantages of less malnutrition and simpler technique compared to other malabsorptive revisional surgeries
Clinical Best Practices
Remove adjustable gastric bands and associated capsules carefully during revisional surgery.
Use a 36 French calibration tube for sleeve creation starting 6 cm from the pylorus.
Fix the sleeved stomach to the diaphragm crus and peripancreatic fascia to prevent migration and twisting.
Perform jejunal anastomosis at approximately one-third of total small bowel length from the duodenojejunal junction to standardize bypass length.
Create a 40-mm stoma using a 45-blue reload stapler and close the defect with two-layer running sutures.
Use orientation stitches to minimize tension, prevent twisting, and reduce reflux risk.
Conduct intraoperative methylene blue leak test to ensure anastomotic integrity.