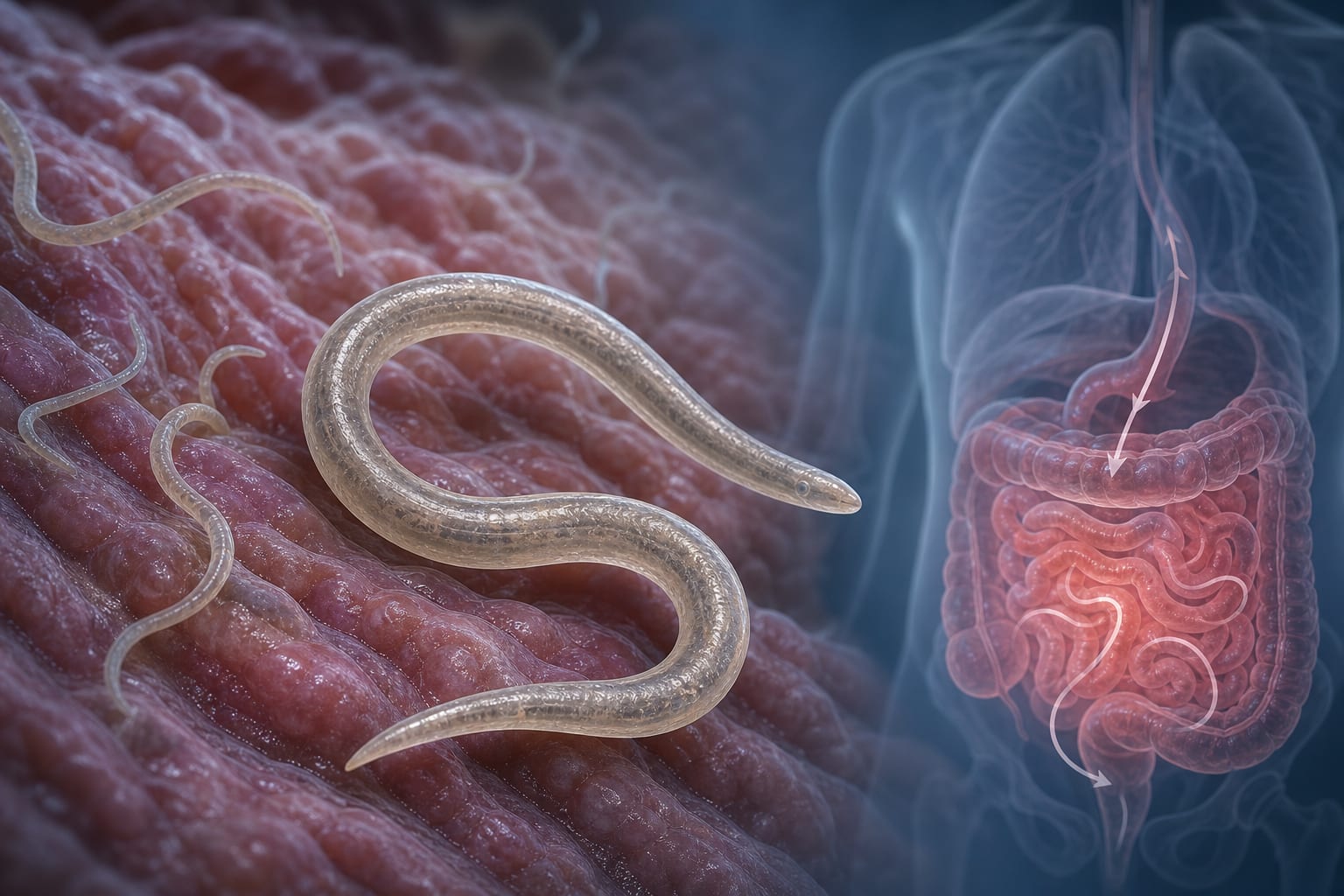
To report a case of Strongyloides stercoralis infection in a 73-year-old female patient, emphasizing the diagnostic challenges and clinical implications of corticosteroid-induced hyperinfection syndrome.
Approach:
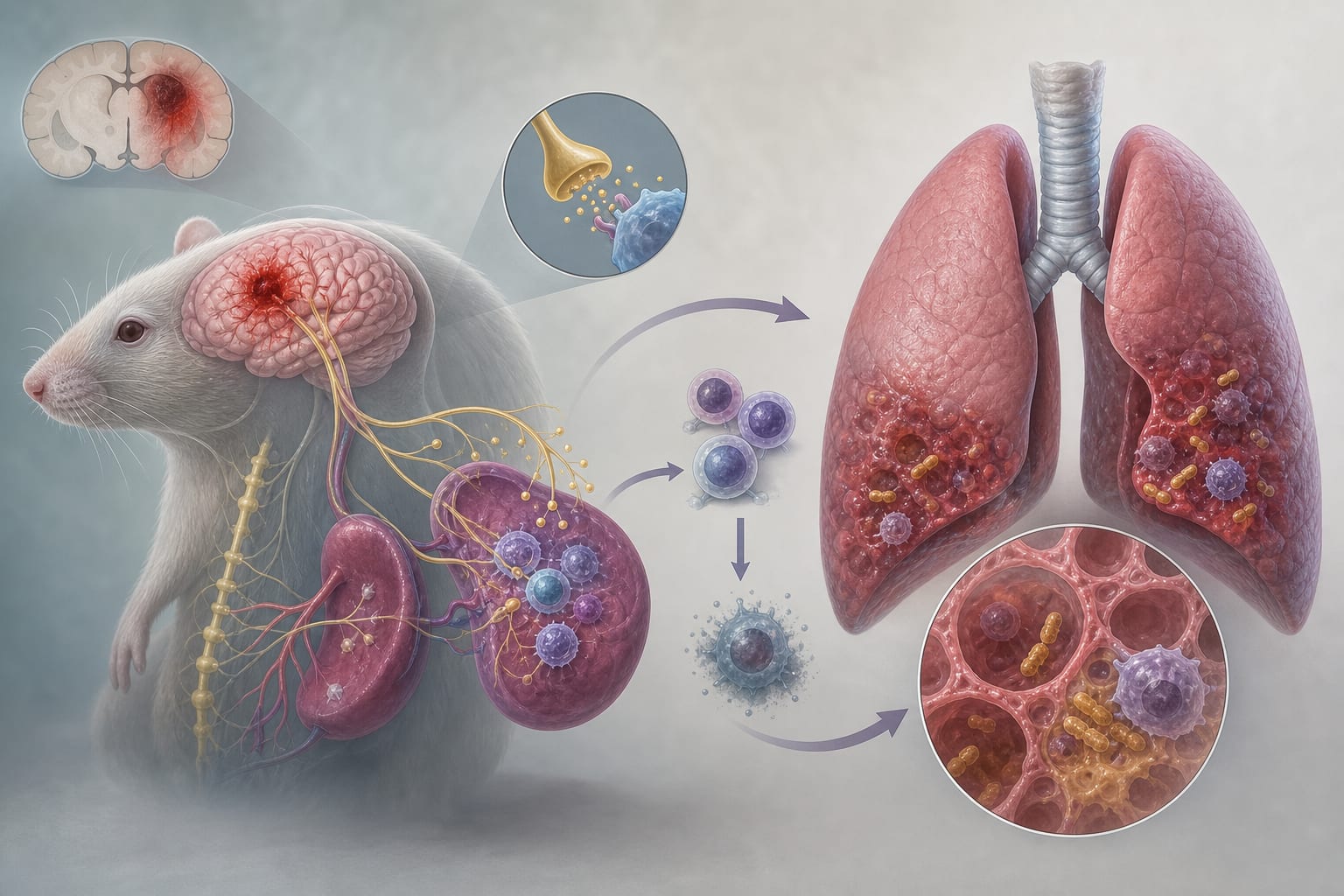
Case Description: A 73-year-old female with a 30-year history of bronchial asthma developed severe hyperinfection syndrome after corticosteroid therapy, initially presenting with cutaneous petechiae and pruritus, followed by gastrointestinal distress.
Diagnostic Process: Diagnosis was confirmed through detection of S. stercoralis in multiple body fluid specimens after initial misdiagnosis and treatment for allergic purpura and fungal infection.
Treatment and Recovery: After discontinuation of corticosteroids and initiation of albendazole, the patient gradually recovered.
Key Findings:
Initial symptoms of S. stercoralis infection can mimic other conditions, leading to diagnostic delays.
Corticosteroid therapy can precipitate hyperinfection syndrome in immunocompromised patients.
Timely discontinuation of immunosuppressive therapy is critical for favorable outcomes.
Interpretation:
The case illustrates the importance of screening for chronic strongyloidiasis in at-risk patients prior to initiating corticosteroid therapy.
Limitations:
The case is a single patient report, limiting generalizability to broader populations.
Diagnostic challenges may differ based on individual patient circumstances.
Conclusion:
Prompt recognition and treatment of disseminated strongyloidiasis are essential to prevent severe outcomes in patients with undiagnosed chronic infections.