Development and validation of a nomogram based on tumor margin irregularity and alpha-fetoprotein for predicting microvascular invasion in hepatocellular carcinoma - Summary - MDSpire
Advertisement
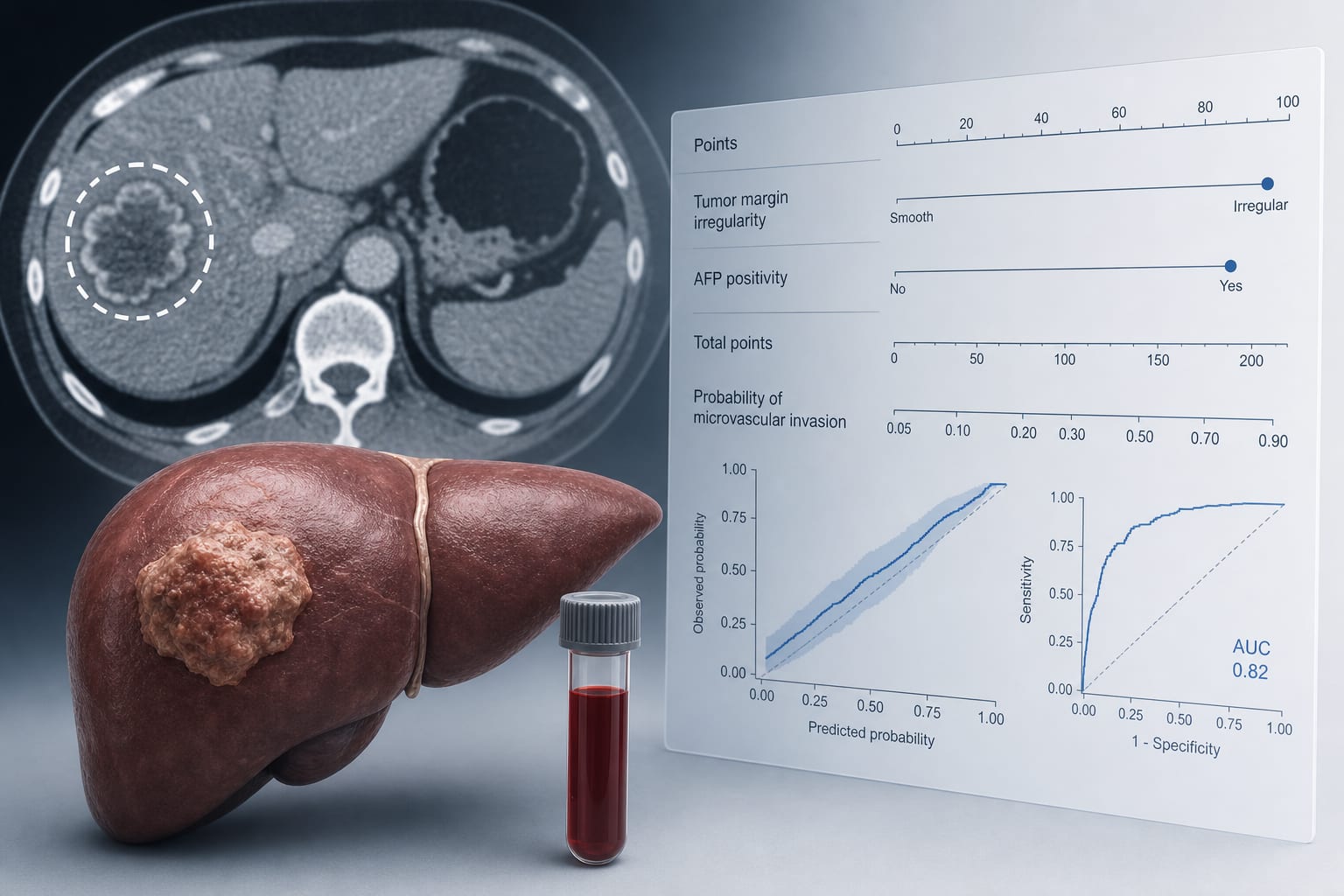
Development and validation of a nomogram based on tumor margin irregularity and alpha-fetoprotein for predicting microvascular invasion in hepatocellular carcinoma
To develop and externally validate a preoperative nomogram based on tumor margin irregularity and alpha-fetoprotein (AFP) positivity for predicting microvascular invasion (MVI) in hepatocellular carcinoma (HCC).
Approach:
Study Design: Retrospective multicenter study with a training cohort of 487 patients and an external validation cohort of 256 patients.
Data Collection: Demographic, clinical, tumor-related, serological, and preoperative CT variables were compared by MVI status.
Analysis Method: LASSO regression for predictor selection followed by multivariable logistic regression; model performance assessed using ROC curves, AUC, calibration, and DCA.
Key Findings:
MVI was present in 187 of 487 patients in the training cohort and 95 of 256 patients in the validation cohort.
LASSO selected AFP positivity, irregular tumor margins, capsular interruption, and intratumoral hyperplastic vessels as predictors.
Irregular tumor margins (adjusted OR = 5.275, 95% CI: 3.165–8.791, p < 0.001) and AFP positivity (adjusted OR = 3.297, 95% CI: 1.983–5.481, p < 0.001) were identified as independent predictors.
The final model achieved AUCs of 0.740 and 0.781 in the training and validation cohorts, respectively.
Interpretation:
The nomogram based on tumor margin irregularity and AFP positivity showed fair-to-acceptable discrimination for preoperative MVI risk stratification in HCC patients.
Limitations:
The study is retrospective and may have selection bias.
External validation was limited to a single cohort.
The model requires further prospective multicenter validation.
Conclusion:
The nomogram may support exploratory preoperative MVI risk stratification in surgically treated or resectable HCC patients.
Harold Burstein, MD, PhD, and Ana C. Garrido-Castro, MD discuss results from the Saci-IO HR+ trial, which were presented at the 2026 ESMO Breast Cancer Congress.