Case report: Central retinal artery occlusion following scleral buckling surgery with secondary angle closure and recurrent acute ocular hypertension - Summary - MDSpire
Advertisement
Case report: Central retinal artery occlusion following scleral buckling surgery with secondary angle closure and recurrent acute ocular hypertension
To report a case of central retinal artery occlusion (CRAO) following combined phacoemulsification and scleral buckling surgery for retinal detachment and to discuss the associated complications.
Approach:
Case Presentation: A man in his late 60s underwent combined phacoemulsification with intraocular lens implantation and segmental scleral buckling for macula-sparing rhegmatogenous retinal detachment caused by inferotemporal ora dialysis. Post-surgery, he experienced recurrent ocular pain, intraocular pressure spikes, anterior chamber shallowing, and visual deterioration.
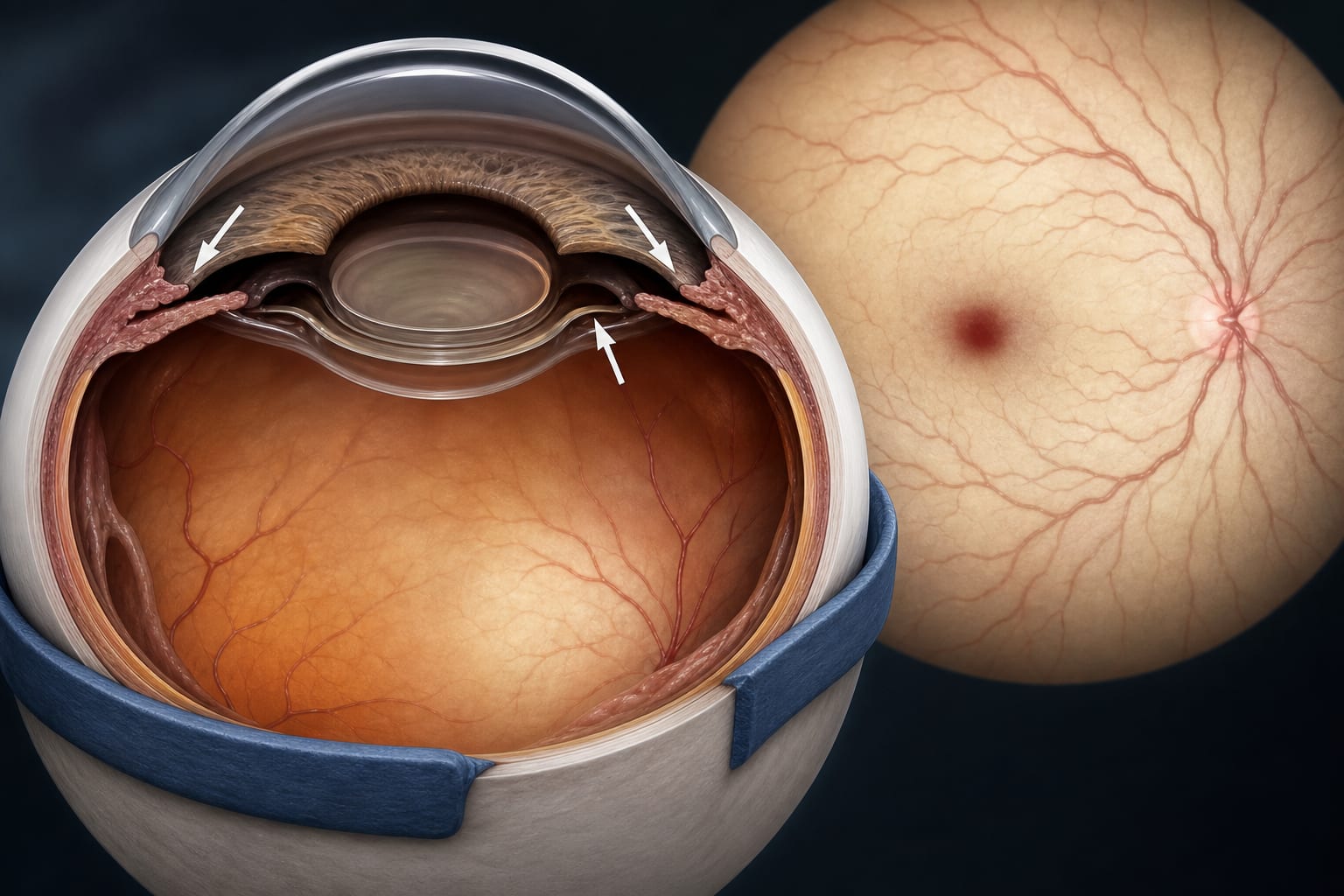
Diagnostic Evaluation: Fundus examination showed diffuse retinal whitening, a cherry-red spot, and marked retinal arterial attenuation. Fluorescein angiography confirmed CRAO with retinal ischemia and choroidal hypoperfusion.
Treatment: The patient received multiple interventions including anterior chamber paracentesis, topical pilocarpine, systemic IOP-lowering therapy, intravenous mannitol, oxygen therapy, and adjunctive supportive treatment.
Key Findings:
The patient developed CRAO shortly after combined phacoemulsification and scleral buckling surgery.
Symptoms included recurrent ocular pain, anterior chamber shallowing, and secondary angle closure.
Visual acuity deteriorated to no light perception despite treatment.
Interpretation:
The case suggests a potential mechanism involving anterior segment crowding due to scleral buckling leading to retinal ischemia.
Limitations:
The mechanism of CRAO could not be definitively proven.
The findings are based on a single patient experience, limiting generalizability.
Conclusion:
Urgent reassessment of IOP and anterior chamber configuration is crucial after scleral buckling surgery when complications arise.
A mission team reflects on surgical innovation, logistical challenges, and the long-term goal of building sustainable vitreoretinal care in West Africa.