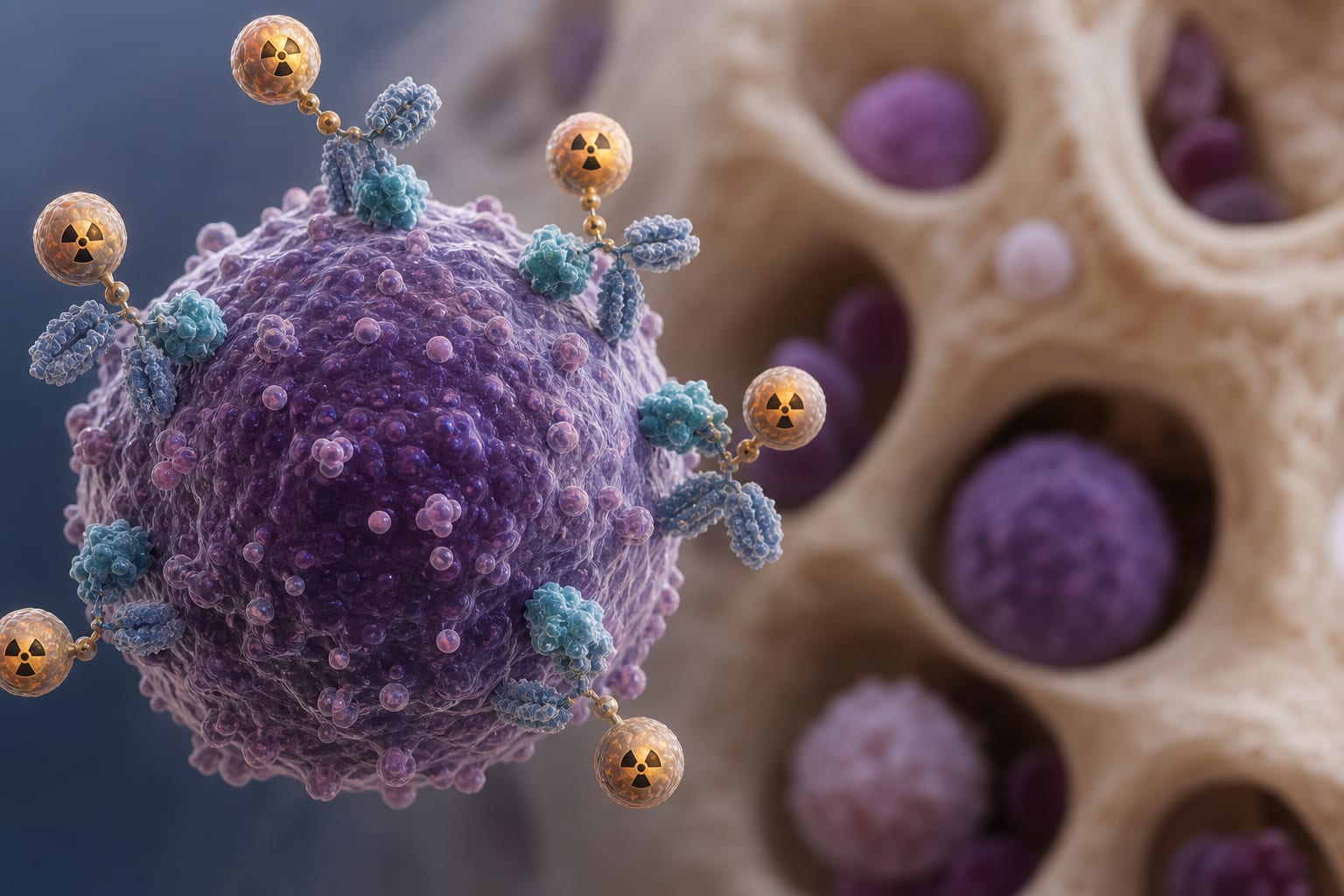
To review the rationale for combining radioimmunotherapy (RIT) with reduced-intensity conditioning (RIC) in allogeneic hematopoietic transplantation (allo-HCT) for leukemia, focusing on antigen selection, radionuclide properties, and clinical experiences related to this combination.
Approach:
Key Findings:
RIT can enhance the efficacy of RIC by delivering targeted radiation to hematopoietic malignancies.
CD45 is the most studied target for RIT, allowing for specific radiation delivery to leukemia cells.
Clinical trials indicate that RIT combined with RIC is feasible and can improve disease control.
Hepatic toxicity is a significant limitation of RIT dosing, necessitating careful organ-specific assessments.
Interpretation:
RIT may improve disease control in RIC allo-HCT without compromising tolerability, but further prospective studies are required to establish its role as a standard component of conditioning.
Limitations:
Current evidence is primarily from early-phase studies, which limits the generalizability of findings.
The role of RIT in the evolving therapeutic landscape of AML and related malignancies is still being defined.
Conclusion:
RIT represents a promising approach for targeted cytoreduction in patients with residual disease at the time of transplantation, warranting further investigation.
Morristown Medical Center now offers patients access to innovative clinical trials for immunotherapies including the use of Chimeric Antigen Receptor T Cells (CAR-T) and Tumor Infiltrating Lymphocytes (TIL).