To explore the historical context and current understanding of Brugada syndrome (BrS) and its future directions.
Approach:
Historical Foundations: Discusses the early recognition of BrS and its electrocardiographic characteristics, paralleling the discovery of Wolff–Parkinson–White syndrome.
Current Understanding: Examines recent advances in recognizing the arrhythmogenic substrate of BrS and the implications for diagnosis and treatment.
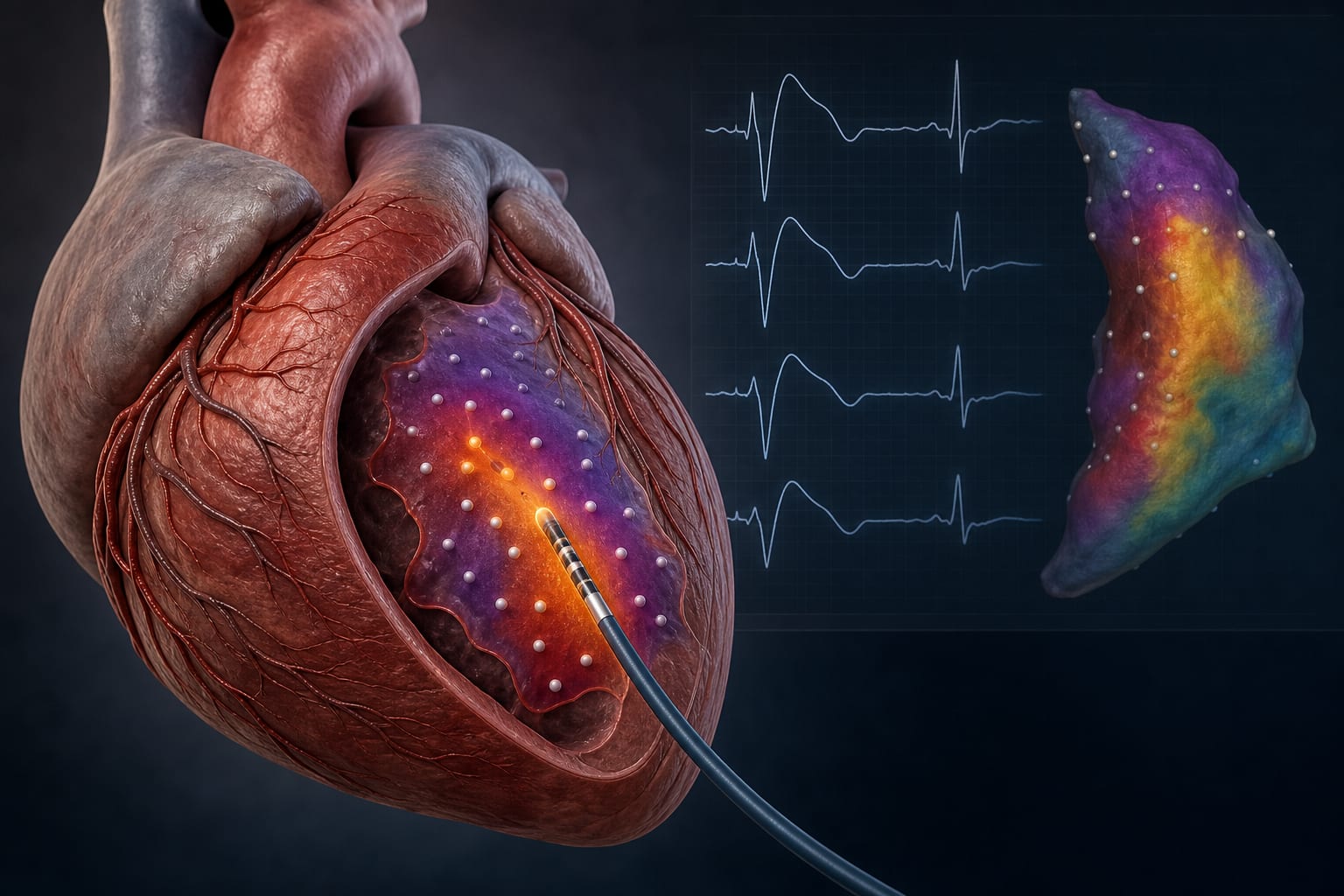
Therapeutic Advances: Highlights the success of epicardial substrate ablation in symptomatic patients and its impact on ECG normalization.
Genetic Understanding: Addresses challenges in genetic testing and the limited specificity of ECG phenotypes in asymptomatic individuals.
Risk Stratification Models: Explores contemporary risk stratification models that integrate various clinical and genetic factors.
Key Findings:
BrS was historically defined by its ECG phenotype, lacking a clearly identifiable substrate.
Recent studies have identified abnormal electrograms in the right ventricular outflow tract as the arrhythmogenic substrate.
Epicardial substrate ablation has shown success in reducing ventricular arrhythmias and normalizing ECG patterns.
Current risk stratification models remain inconsistent, particularly for asymptomatic patients.
Interpretation:
Understanding of BrS has evolved from a focus on electrocardiographic features to recognizing the significance of the underlying arrhythmogenic substrate.
Limitations:
Risk stratification in asymptomatic individuals remains challenging due to limited specificity of ECG phenotypes.
Genetic testing yields pathogenic variants in only a minority of patients.
Conclusion:
Ongoing research is essential to refine diagnostic criteria and enhance risk stratification in BrS.
Shear wave velocity measurements in the basal anteroseptal and right ventricular walls differed between transthyretin and light chain cardiac amyloidosis when conventional echocardiographic parameters did not.