To conceptualize SCAD as a disorder of coronary wall integrity and evaluate its molecular basis, clinical recognition, and management complexities.
Approach:
Framework Development: Developed a provisional framework that integrates evidence to understand SCAD as a disorder of coronary wall integrity, focusing on its complex pathophysiology.
Critical Evaluation: Evaluated models of SCAD initiation, including genetic factors and management controversies, through a systematic review of existing literature.
Research Roadmap Proposal: Proposed a roadmap for future research that emphasizes the need for multiomic cohorts and high-resolution imaging to better understand SCAD.
Key Findings:
SCAD is a significant cause of myocardial infarction in young and middle-aged women, often under-recognized in clinical settings.
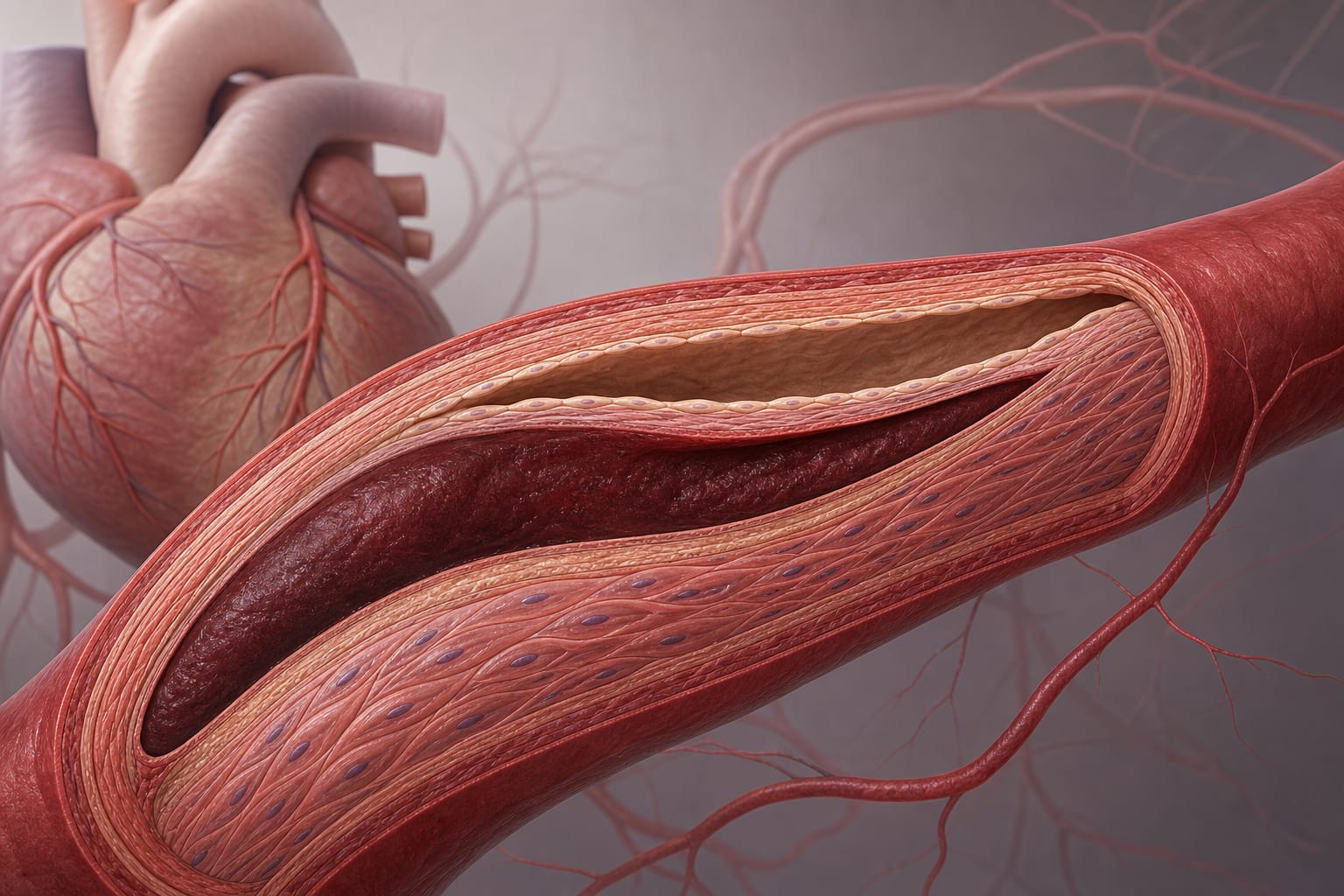
The final pathological event in SCAD is intramural hematoma formation and true-lumen compression, which can lead to severe ischemic events.
SCAD is influenced by inherited susceptibility, extracellular matrix architecture, and various hemodynamic factors, highlighting its multifactorial nature.
Interpretation:
SCAD should be understood as a complex disorder influenced by multiple factors, necessitating a nuanced approach to diagnosis and management.
Limitations:
The molecular basis of SCAD remains incompletely understood, with ongoing research needed to clarify its pathophysiology.
Current diagnostic frameworks may not fully capture the complexity of SCAD, potentially leading to misdiagnosis or delayed treatment.
Conclusion:
A threshold model for SCAD organizes current evidence and highlights the need for further research to enhance understanding and management strategies.