Percutaneous nephrostomy as a marker of clinical vulnerability in non-metastatic muscle-invasive bladder cancer: prognostic and infectious implications - Summary - MDSpire
Advertisement
Percutaneous nephrostomy as a marker of clinical vulnerability in non-metastatic muscle-invasive bladder cancer: prognostic and infectious implications
To evaluate the association between percutaneous nephrostomy (PCN) at diagnosis and clinical outcomes in patients with non-metastatic muscle-invasive bladder cancer (MIBC).
Key Findings:
PCN was present in 27.1% of patients, indicating a significant portion of the cohort.
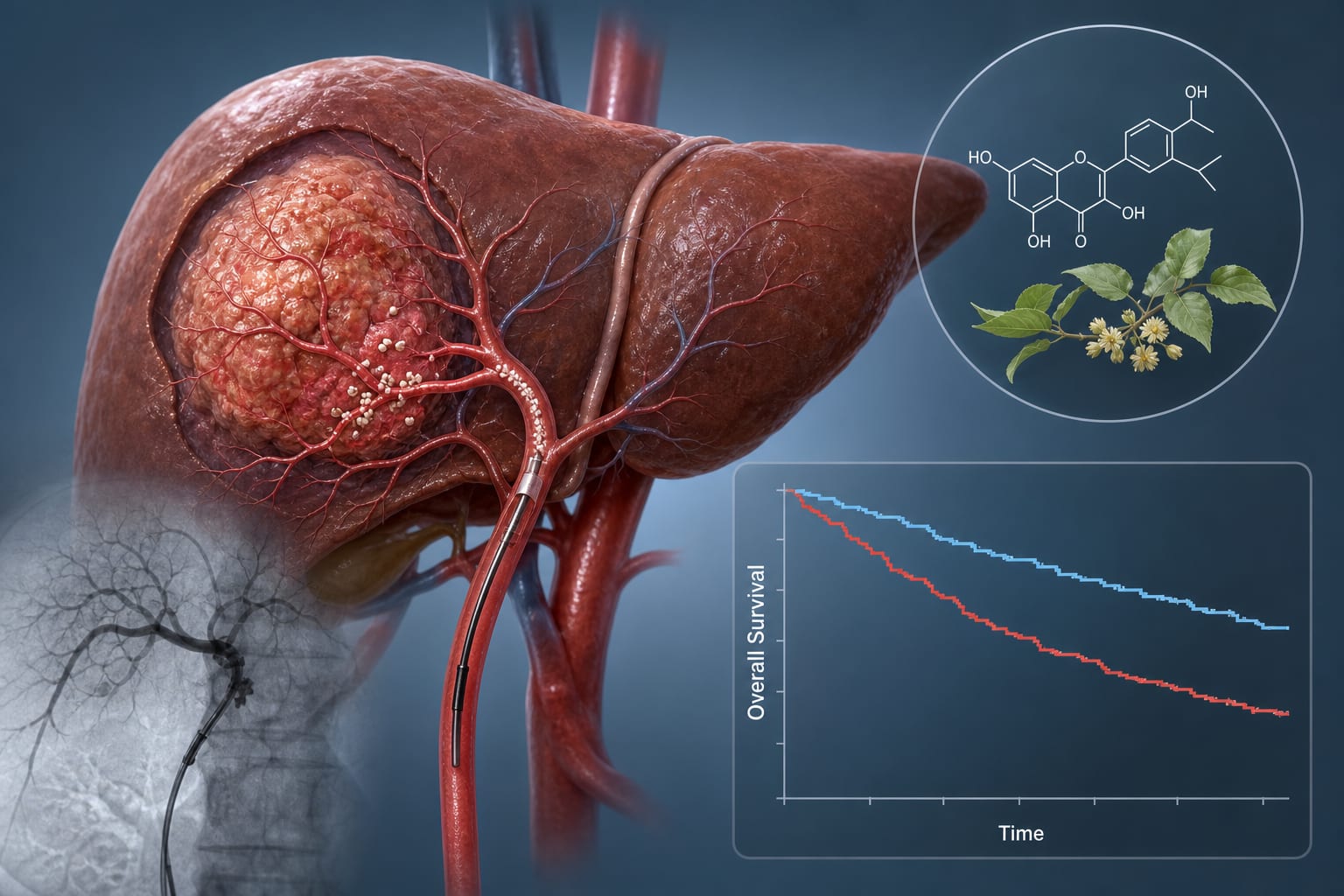
Median OS was shorter in the PCN group (24 months) compared to non-PCN (41 months, p = 0.004), highlighting a potential survival disadvantage.
PCN did not retain independent prognostic significance after adjustment for covariates (HR 0.433; p = 0.069), suggesting other factors are more critical.
ECOG performance status, CRP, and N stage were identified as independent predictors of OS, emphasizing their importance in prognosis.
PCN was a strong predictor of positive urine cultures (OR 2.685; p = 0.038) and infection-related hospitalizations (OR 13.995; p < 0.001), indicating a significant risk of infectious complications.
Interpretation:
PCN was not an independent predictor of OS after adjustment, suggesting that the observed survival disadvantage reflects baseline clinical vulnerability rather than a direct effect of the procedure. However, PCN was independently associated with increased infectious morbidity, underscoring the need for careful evaluation and management.
Limitations:
Retrospective design may introduce bias.
Findings may not be generalizable beyond the studied population.
Conclusion:
PCN serves as a marker of clinical frailty, necessitating careful evaluation before placement and proactive management of infectious complications.