To delineate current standards in colon cancer resection regarding longitudinal margins, lymphadenectomy, and mesenteric excision.
Approach:
Key Findings:
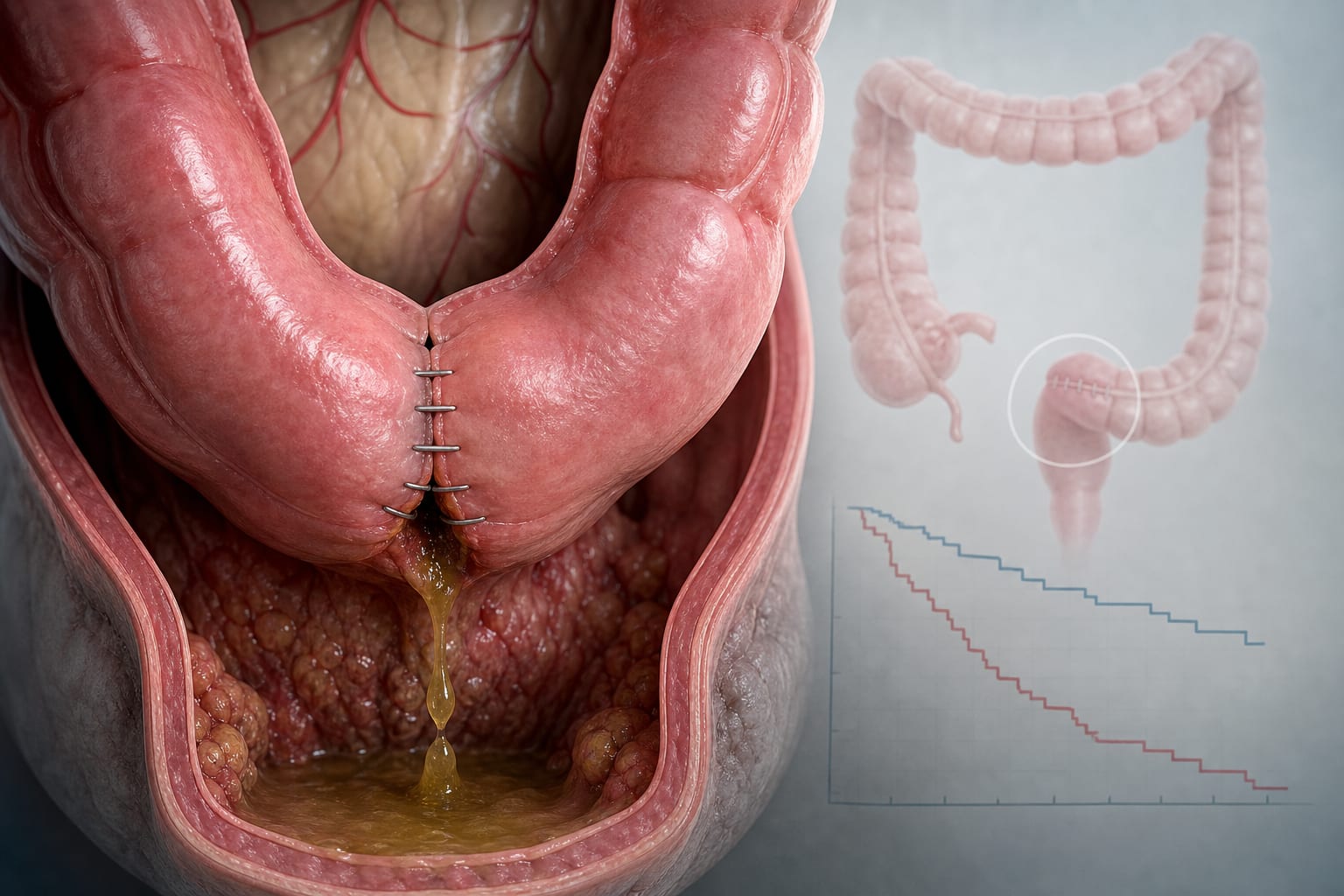
Optimal longitudinal margins for most tumors are 5–7 cm, extending to 10 cm for advanced T stage (cT3–cT4) or specific arterial geometry.
Lymph node assessment beyond the historical minimum of 12 nodes improves staging accuracy and survival, with a plateau around 18–22 examined nodes.
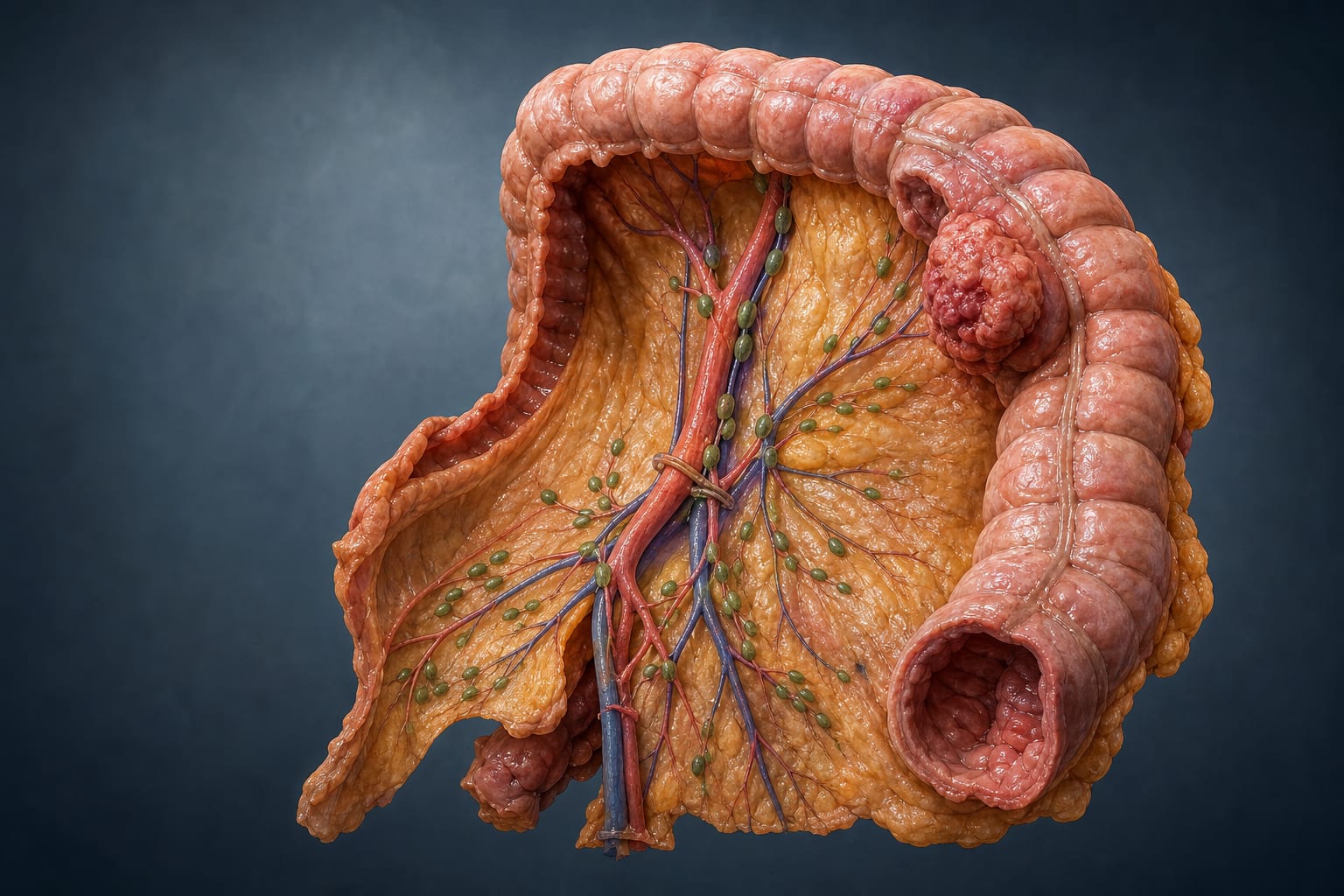
Complete mesocolic excision (CME) with central vascular ligation (CVL) increases nodal yield and specimen quality without excess morbidity and shows oncologic advantage particularly in stage III disease.
Interpretation:
An oncologically adequate colectomy should aim for R0 resection with appropriate margins, mesenteric resection to the feeding-vessel origin, and systematic lymph node assessment.
Limitations:
Heterogeneity in international standards and practices regarding colon cancer resection.
Variability in definitions and classifications of pericolic lymph nodes across different guidelines.
Conclusion:
An adequate colectomy should target specific margins, lymph node yields, and incorporate CME/CVL/D3 techniques, particularly for stage III right colon cancers.
by Mariarosaria Portinaio, Carlo Alberto Schena, Michele Ammendola, Geoffrey Yuet Mun Wong, Patricia Tejedor, Fausto Rosa, Elisa Reitano, Corrado Pedrazzani, Jim Khan, Nicola de’Angelis