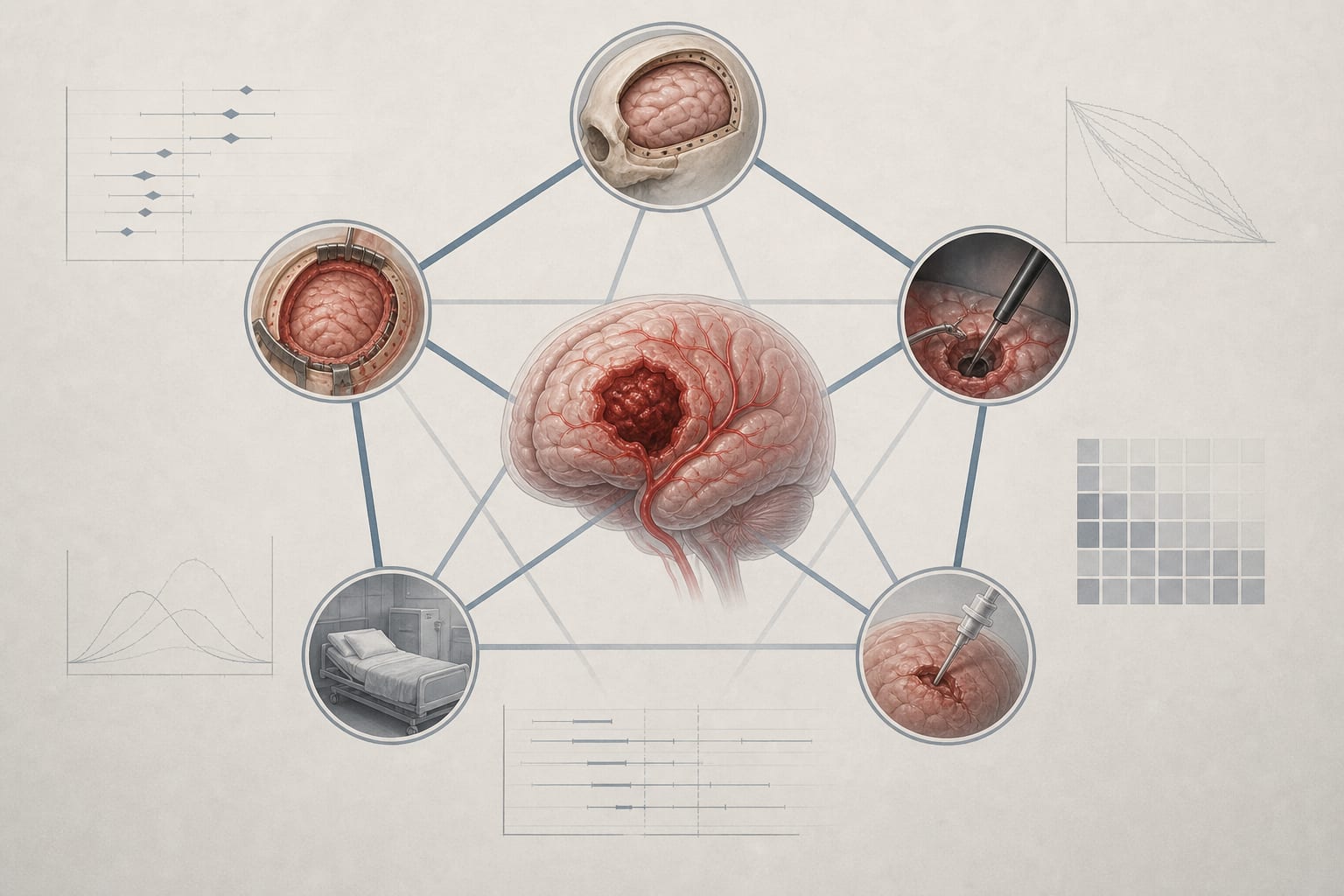
To compare the efficacy and perioperative outcomes of conservative medical treatment (CMT) and surgical interventions—including decompressive craniectomy (DC), craniotomy (CC), endoscopic surgery (ES), and minimally invasive puncture surgery (MIPS)—in patients with spontaneous intracerebral hemorrhage (ICH).
Approach:
Key Findings:
MIPS and ES ranked highest for good functional outcome at 6 months, significantly superior to CC and CMT.
DC ranked highest for 6-month mortality, though most pairwise comparisons did not reach statistical significance.
ES and MIPS significantly reduced operative time and intraoperative blood loss compared to CC.
Interpretation:
MIPS and ES may provide advantages in functional recovery and perioperative burden, while DC may offer potential survival benefits; however, the evidence remains uncertain and requires cautious interpretation.
Limitations:
Current evidence is limited and requires further high-quality multicenter randomized trials to clarify the role of DC.
Direct head-to-head randomized evidence comparing multiple surgical strategies is lacking.
Conclusion:
Clinical decision-making should balance long-term outcomes against perioperative trade-offs and be individualized according to disease severity and patient-specific risk factors.