To develop and internally validate a clinical prediction model for adverse pregnancy outcomes in women with early-onset preeclampsia (EOPE).
Approach:
Key Findings:
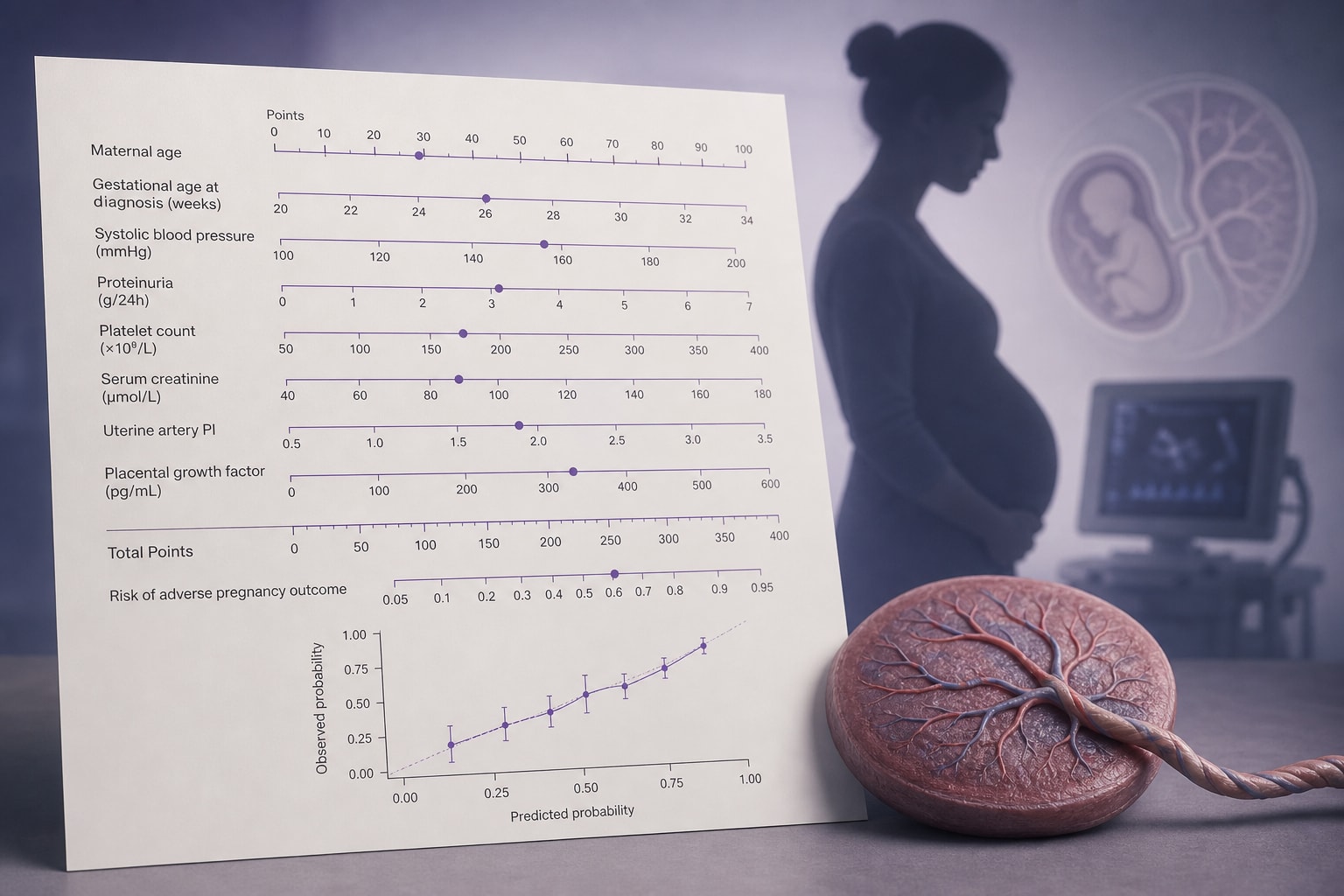
Seven independent predictors identified: gestational age at admission, systolic blood pressure, urine protein score, platelet count, AST level, fetal growth restriction, and HELLP syndrome.
The nomogram showed good discrimination with an AUC of 0.859 in the validation cohort.
Calibration curves indicated acceptable agreement between predicted and observed risks.
Interpretation:
The nomogram is intended for admission-based risk stratification after EOPE diagnosis, not for early prenatal prediction or initial occurrence of EOPE.
Limitations:
The model requires independent multicenter validation before clinical implementation.
Risk categories proposed are exploratory and should not be used as definitive clinical decision cutoffs.
Conclusion:
The study developed a nomogram-based prediction model for adverse pregnancy outcomes in women with EOPE, demonstrating good predictive performance in a single-center cohort.