To explore the effect of laparoscopic ovarian cystectomy on ovarian reserve function and its related risk factors.
Approach:
Key Findings:
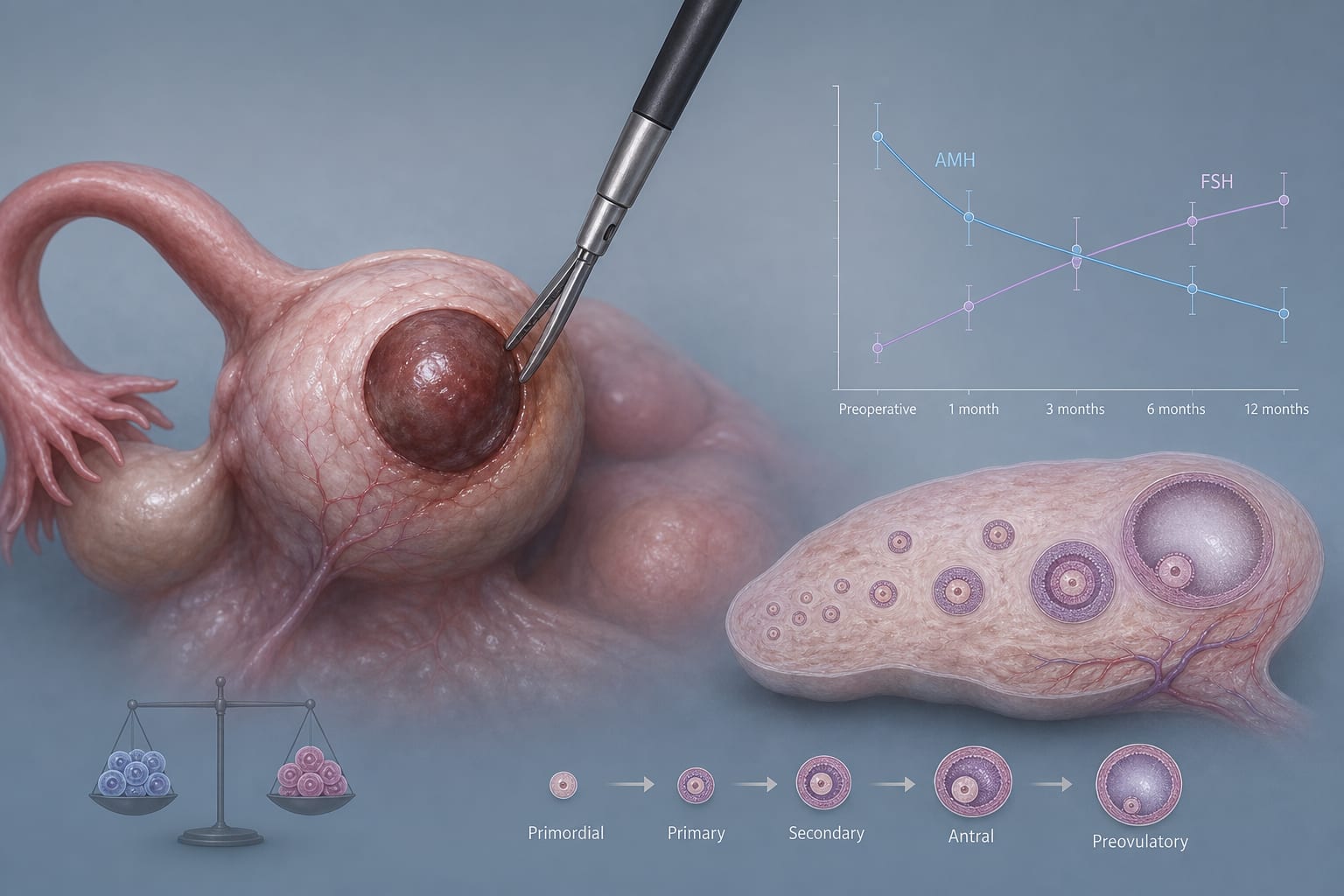
At 1, 3, 6, and 12 months after surgery, the AMH levels were significantly lower than those before surgery, while the FSH levels were higher than those before surgery (P < 0.05).
At 12 months after surgery, the decrease in AMH levels and the increase in FSH levels in the cyst diameter ≥7 cm group were significantly greater than those in the cyst diameter <5 cm and 5 − 7 cm groups (P < 0.001).
The decrease in AMH and the increase in FSH in the electrocoagulation hemostasis group were significantly greater than those in the suture hemostasis group (P < 0.05).
Among 86 patients with fertility intentions, the overall pregnancy rate was 59.3% (51/86), and the live birth rate was 48.8% (42/86).
Multivariable logistic regression analysis showed that cyst diameter ≥7 cm (OR = 3.610, 95%CI: 1.835 − 7.103), endometriotic cysts (OR = 2.063, 95%CI: 1.106–3.848), electrocoagulation hemostasis (OR = 2.633, 95%CI: 1.232 − 5.627), and moderate-to-severe ovarian tissue loss (OR = 4.697, 95%CI: 2.312 − 9.545) were independent risk factors for significant postoperative AMH decrease (≥30%) (P < 0.05).
Interpretation:
Laparoscopic ovarian cystectomy leads to a decrease in ovarian reserve function, indicated by lower AMH and higher FSH levels, with recovery over time.
Limitations:
Retrospective design may introduce selection bias.
Limited to patients with unilateral ovarian cysts.
Conclusion:
Laparoscopic ovarian cystectomy causes some damage to ovarian reserve function, with specific factors influencing the degree of impact.
A two-marker methylated DNA assay identified endometrial cancer with 96% sensitivity in self-collected vaginal fluid — but prospective validation is needed before it can reduce biopsies in routine care.