Risk stratification model based on estimated dose of radiation to immune cells and radiotherapy-related nadir lymphocyte count for predicting the efficacy of consolidation immunotherapy in stage III non-small cell lung cancer - Summary - MDSpire
Advertisement
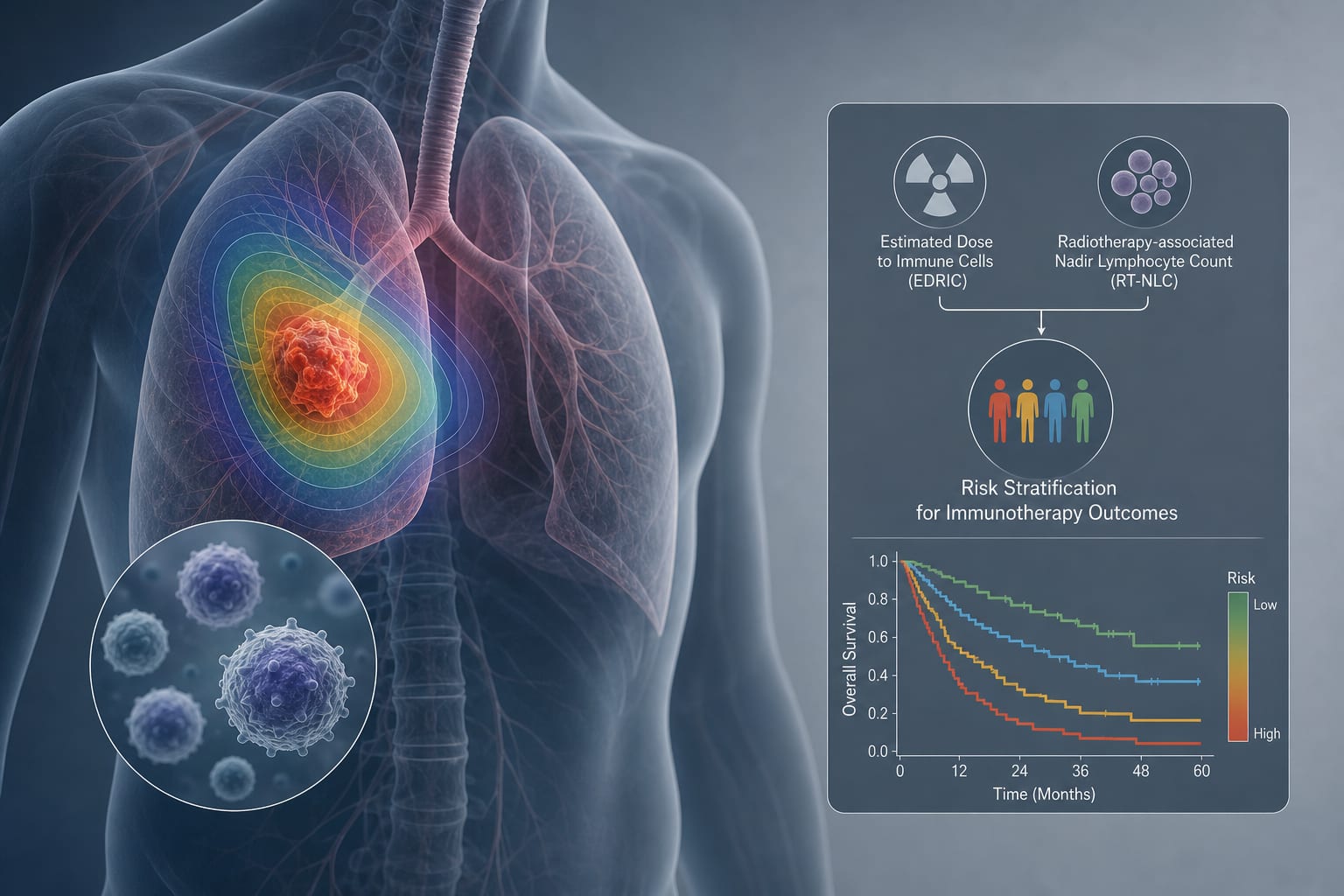
Risk stratification model based on estimated dose of radiation to immune cells and radiotherapy-related nadir lymphocyte count for predicting the efficacy of consolidation immunotherapy in stage III non-small cell lung cancer
To evaluate the prognostic value of estimated dose of radiation to immune cells (EDRIC) and radiotherapy-related nadir lymphocyte count (RT-NLC) for predicting outcomes in patients with unresectable stage III non-small cell lung cancer (NSCLC) treated with definitive chemoradiotherapy and immunotherapy.
Approach:
Risk Stratification: High-risk patients were defined as having EDRIC ≥ 6.75 Gy and RT-NLC < 0.54×10^9/L.
Key Findings:
EDRIC inversely correlated with RT-NLC (r = -0.38, P < 0.001).
Lower EDRIC was associated with significantly improved median overall survival (OS: 49.7 vs. 38.1 months, P = 0.015), progression-free survival (PFS: 29.7 vs. 17.3 months, P = 0.006), locoregional relapse-free survival (LRFS: 32.4 vs. 19.8 months, P = 0.004), and distant metastasis-free survival (DMFS: 44.8 vs. 24.0 months, P = 0.001).
High RT-NLC group showed prolonged median distant metastasis-free survival (DMFS: 44.8 vs 26.8 months, P = 0.012).
High-risk patients demonstrated inferior survival (P < 0.05) but derived significant benefit from consolidation immunotherapy, with improved OS (HR = 0.37, P = 0.041), PFS (HR = 0.44, P = 0.034), and DMFS (HR = 0.33, P = 0.011).
Interpretation:
EDRIC and RT-NLC are significant prognostic biomarkers in unresectable stage III NSCLC.
Limitations:
Retrospective design may introduce bias.
Single-center study limits generalizability.
Need for prospective validation of findings.
Conclusion:
The study supports the identification of high-risk patients who may benefit from consolidation immunotherapy.