Effects of mandibular advancement devices vs. CPAP on blood pressure in obstructive sleep apnea: a systematic review and meta-analysis of randomized controlled trials - Summary - MDSpire
Advertisement
Effects of mandibular advancement devices vs. CPAP on blood pressure in obstructive sleep apnea: a systematic review and meta-analysis of randomized controlled trials
To systematically evaluate and compare the effects of mandibular advancement devices (MAD) vs. CPAP and inactive controls on blood pressure (BP), sleep-related respiratory events, and treatment adherence in patients with OSA, emphasizing the importance of adherence in treatment outcomes.
Key Findings:
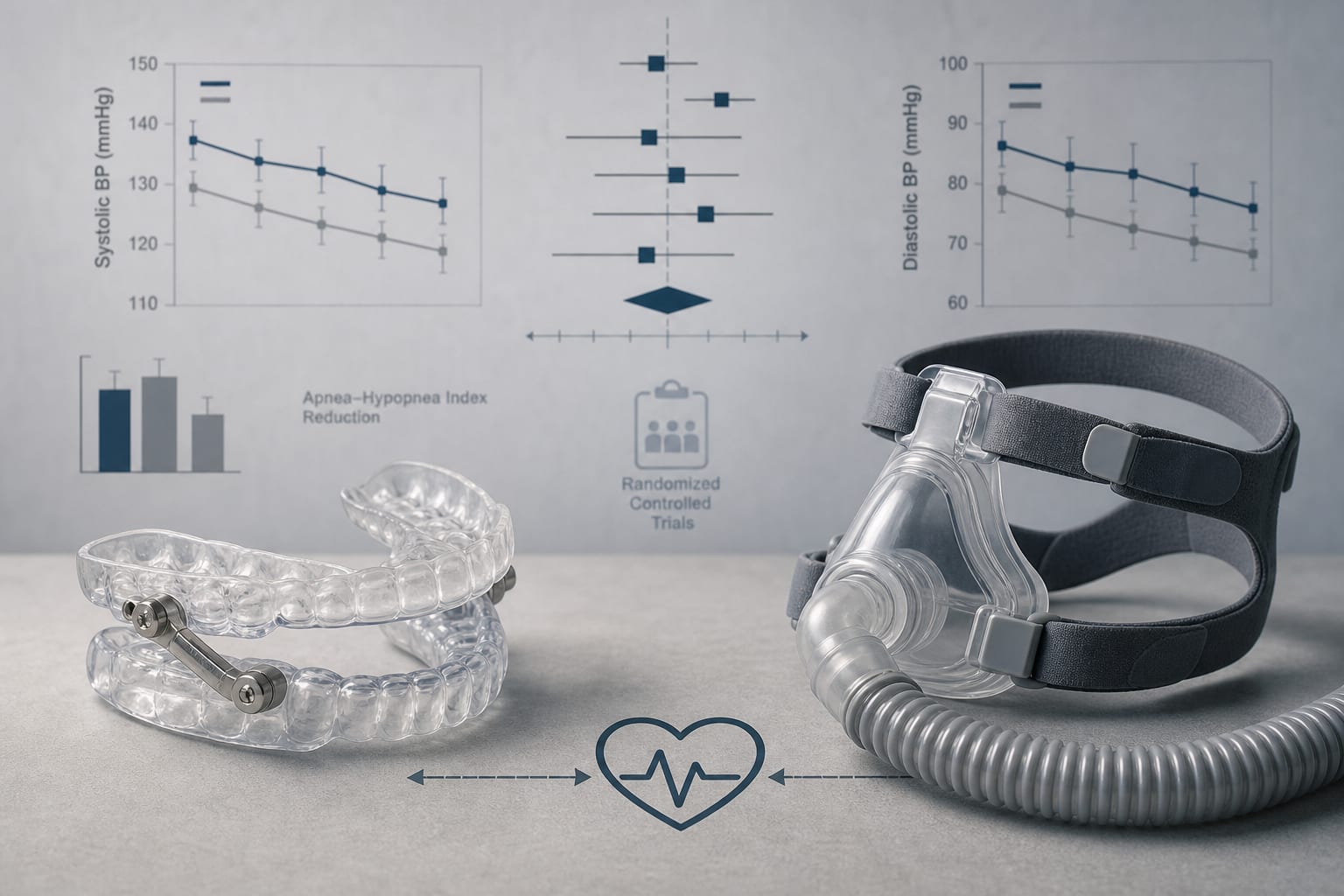
MAD showed overall trends of BP reduction compared to inactive controls across 14 RCTs with 1,141 patients.
MAD achieved a significantly greater reduction in daytime systolic BP compared to CPAP (MD = -1.99 mmHg, p = 0.03).
CPAP demonstrated superior efficacy in reducing AHI (MD = 8.45 events/h, p < 0.001).
MAD and CPAP yielded comparable improvements in subjective sleepiness (ESS).
MAD had significantly longer nightly adherence than CPAP (MD = 0.71 h/night, p < 0.001).
Interpretation:
MAD offers cardiovascular benefits comparable to CPAP and shows a significant reduction in daytime SBP, potentially due to better adherence, making it a viable alternative for patients intolerant to CPAP, with implications for clinical practice.
Limitations:
The physiological inferiority of MAD in reducing AHI compared to CPAP.
Variability in device design and treatment duration may influence outcomes.
Potential biases in study selection and data reporting.
Conclusion:
MAD may serve as an effective alternative for cardiovascular risk management in OSA patients who cannot tolerate CPAP, highlighting its importance in treatment strategies.
A four-factor staging system stratified response rates from 90.9% to 37.5% in a retrospective cohort study, although the model showed only moderate discrimination (C statistic, 0.68) and requires external validation
In a target-trial emulation of more than 600,000 veterans, GLP-1 RA initiators saw fewer new substance use disorders—and patients with existing SUDs had fewer overdoses, hospitalizations, and deaths.