Adjunctive role of p16/Ki-67 dual-stain cytology in colposcopy referral pathways for cervical precancer and persistent high-risk HPV infection - Summary - MDSpire
Advertisement
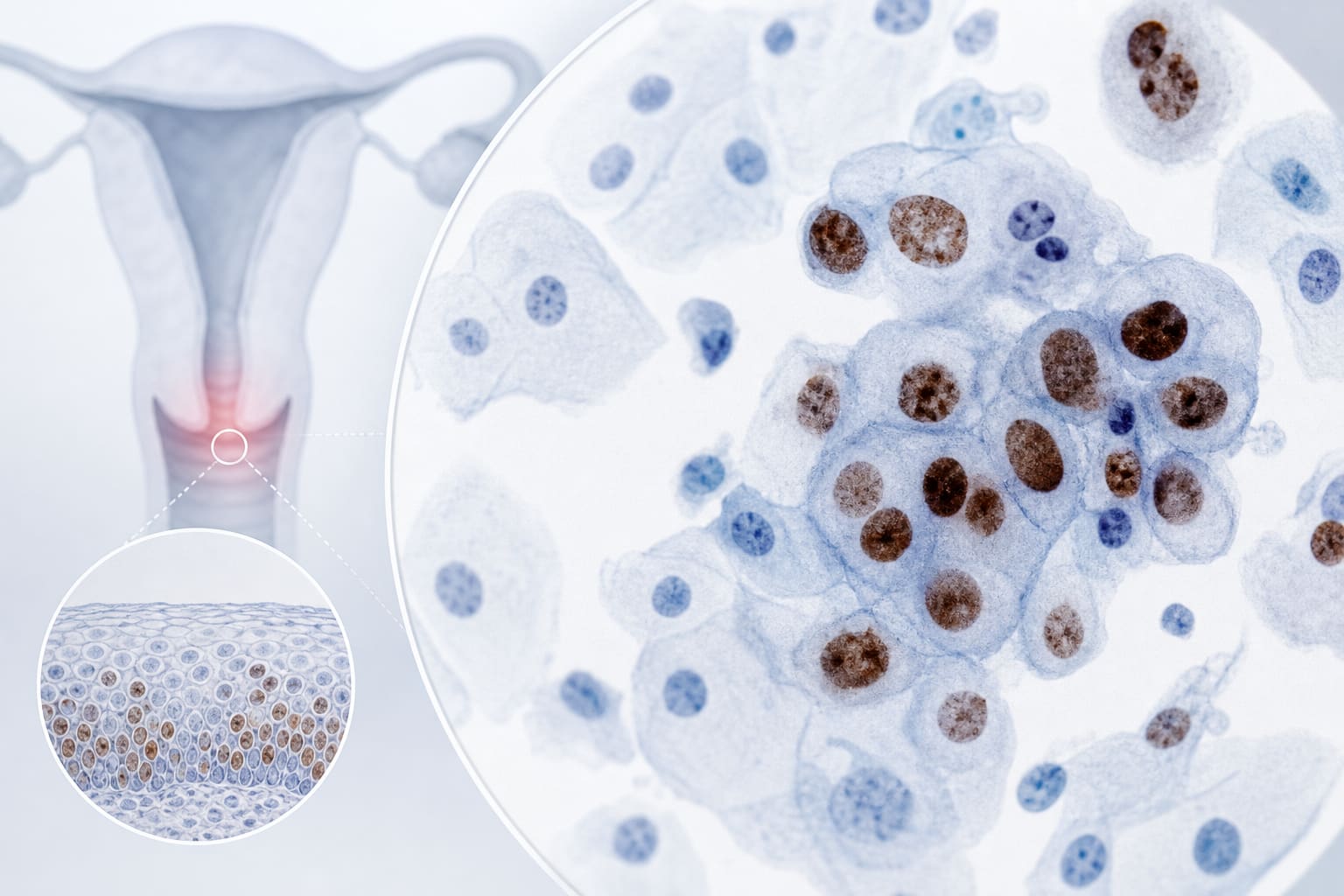
Adjunctive role of p16/Ki-67 dual-stain cytology in colposcopy referral pathways for cervical precancer and persistent high-risk HPV infection
To evaluate the adjunctive triage performance of p16/Ki-67 dual staining cytology for cervical lesions in a colposcopy-referred cohort, analyze its correlation with lesion severity, and explore its predictive value for persistent high-risk HPV infection.
Approach:
Study Design: 109 patients undergoing colposcopic cervical biopsy were included, evaluated for the diagnostic performance of p16/Ki-67 dual-stain cytology.
Testing: Patients underwent HPV, TCT, and p16/Ki-67 DS testing prior to biopsy.
Follow-up: Among HR-HPV-positive patients with CIN1 or lower lesions, follow-up was conducted for 6 months to assess persistent infection.
Key Findings:
Positivity rate of p16/Ki-67 DS cytology increased with cervical lesion severity (P<0.001).
Sensitivity, specificity, accuracy, and AUC for CIN2+ were 77.8%, 88.6%, 84.4%, and 0.822 ± 0.052.
For CIN3+, these metrics were 93.3%, 81.3%, 81.7%, and 0.823 ± 0.056.
87.1% of DS-positive patients with HR-HPV-positive CIN1/lower lesions had persistent infection compared to 62.9% of DS-negative patients (P = 0.025), with an odds ratio of 4.515 (P = 0.028).
Interpretation:
p16/Ki-67 dual-stain cytology demonstrated satisfactory triage efficacy for identifying CIN2+ and CIN3+, and predicted persistent HR-HPV infection in patients with ≤CIN1 lesions.
Limitations:
All analyses are limited to diagnostic efficacy in the referral cohort.
Potential clinical applications, including possible reductions in unnecessary procedures, remain exploratory hypotheses that require prospective clinical validation.
Conclusion:
Further investigation is warranted into the role of p16/Ki-67 dual-stain cytology in cervical cancer screening.