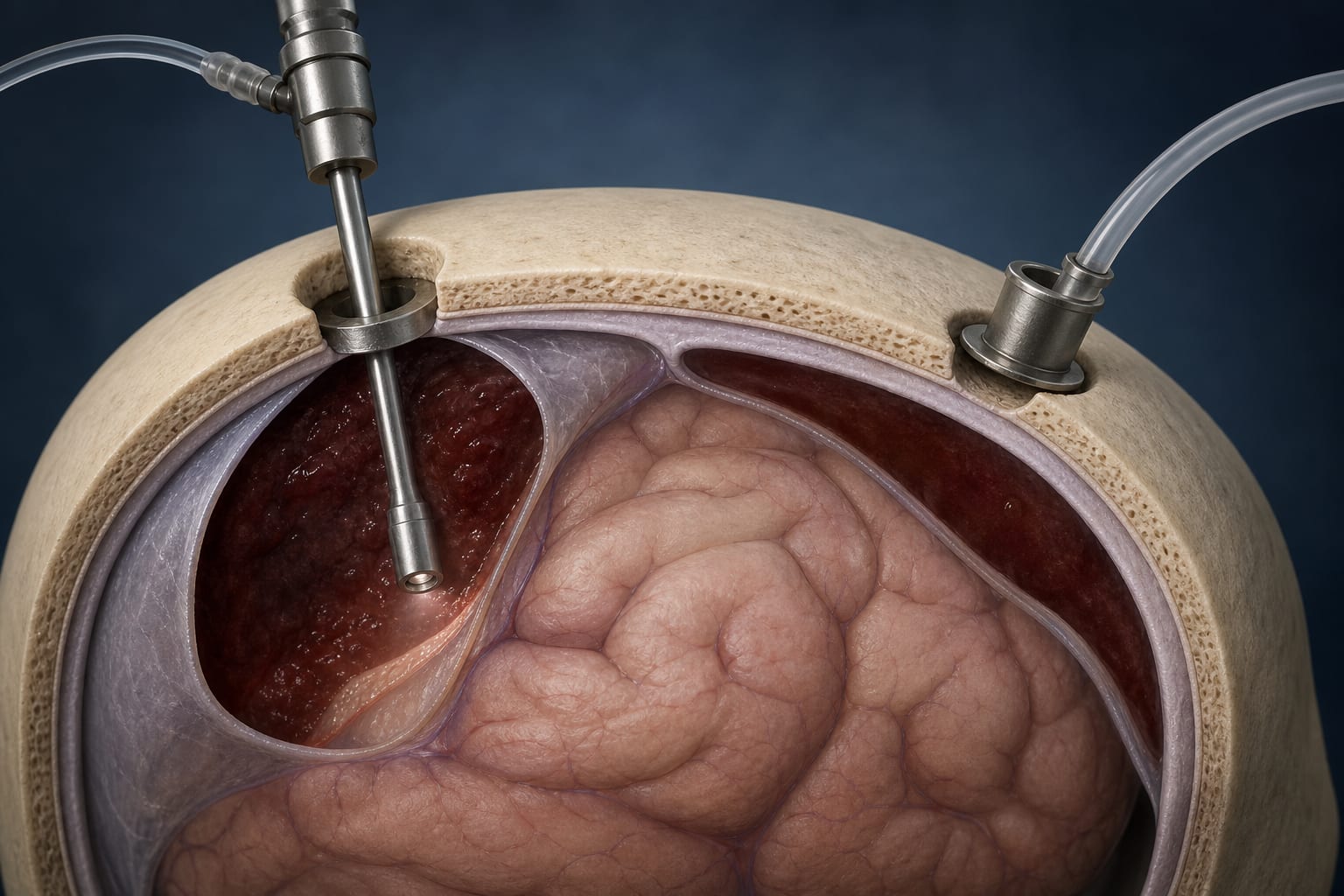
To evaluate the perioperative results of endoscopic-assisted evacuation compared to burr-hole drainage techniques in chronic subdural hematoma (CSDH), emphasizing the comparative aspect.
Key Findings:
Endoscopic-assisted evacuation resulted in significantly lower residual hematoma rates (35.00% vs. 54.78%, p = 0.0255).
Enhanced neurological outcomes were observed in the endoscopic group (odds ratio 0.30, 95% CI: 0.12–0.63, p = 0.0021).
Endoscopic procedures had longer operative times (average 40.12 min longer, p < 0.0001) and higher hospitalization costs (average ¥9,600 more, p < 0.0001).
Postoperative complication rates were similar between both groups.
Interpretation:
Endoscopic-assisted evacuation offers better hematoma removal and neurological recovery without increasing postoperative complications; however, its higher costs may limit accessibility and impact clinical decision-making.
Limitations:
Single-center study may limit generalizability and applicability to broader populations.
Retrospective design may introduce selection bias, affecting the reliability of the findings.
Conclusion:
Endoscopic-assisted evacuation is more effective in managing CSDH compared to burr-hole drainage, though its cost may restrict its use in some settings, highlighting the need for careful consideration in clinical practice.
These 10 states make it more practical for physicians to participate in hospital ownership by aligning statutory structure, corporate practice of medicine rules, and population trends.