To develop an algorithm based on a CHAID decision tree for the structured risk stratification of rare rheumatic diseases in a tertiary referral setting with unclear systemic complaints.
Approach:
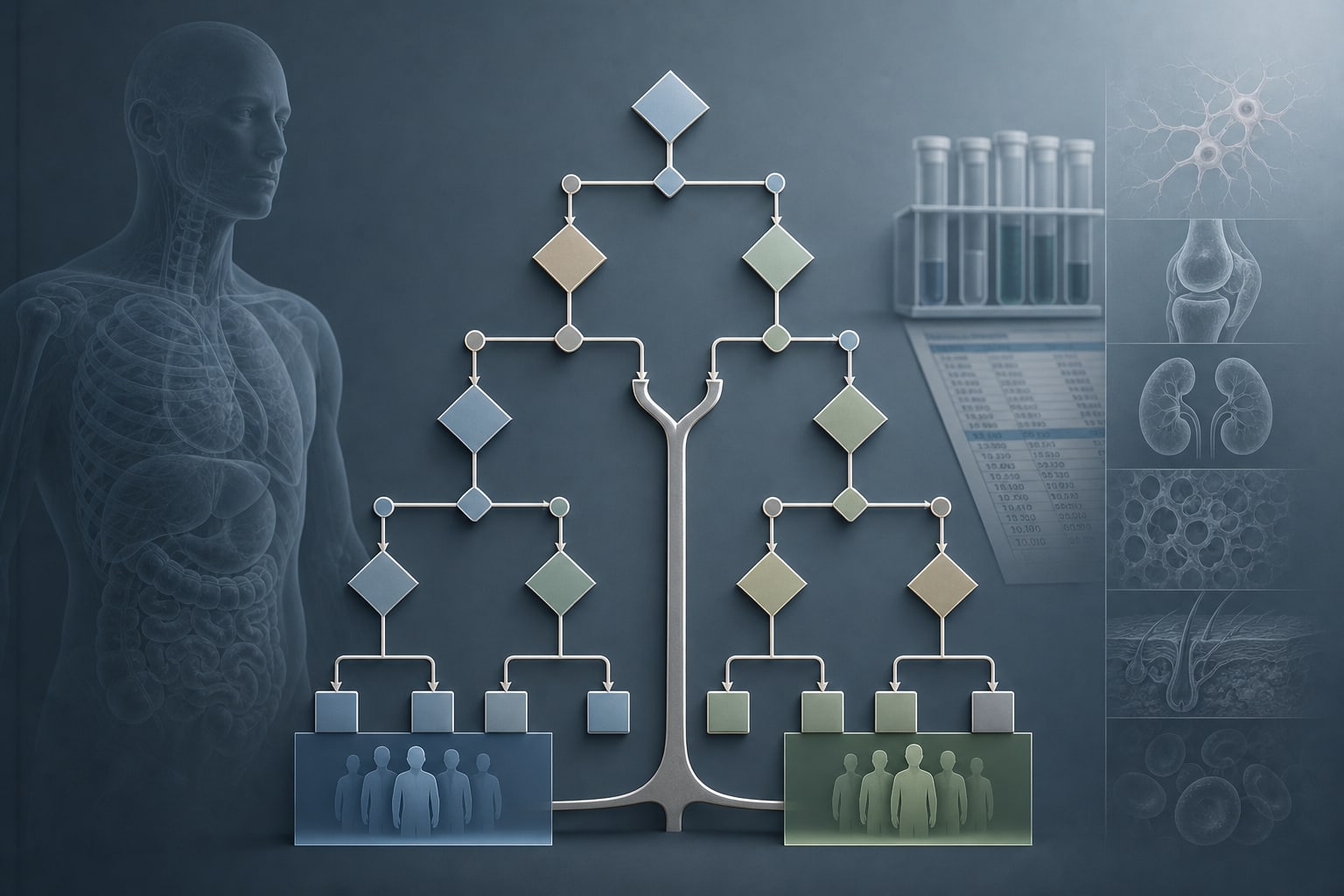
Statistical Analysis: Group differences were analyzed descriptively using inferential statistics, including t-tests and chi-square tests, and a CHAID decision tree model was constructed for risk stratification.
Key Findings:
52.0% of patients received a confirmed rheumatologic diagnosis.
Fatigue and generalized pain were the most prevalent symptoms across diagnostic groups.
The RHEUMA group had significantly higher scores in selected symptom domains and an immunoserological laboratory index.
The CHAID-based decision model achieved an apparent classification of 81.5% (AUC = 0.893), outperforming logistic regression (76.3%, AUC = 0.823).
Interpretation:
The decision tree model provides a framework for structured risk stratification in a tertiary referral population, illustrating the use of symptom aggregation to support clinical reasoning.
Limitations:
Monocentric, retrospective, and exploratory study design, which may limit the generalizability of the findings.
Findings should be interpreted as hypothesis-generating, necessitating further research.
External validation in independent cohorts is required for assessing model generalizability.
Conclusion:
The approach illustrates the potential of structured clinical reasoning in complex multisystem presentations, while acknowledging the need for further validation.
In a nationwide Finnish cohort, patients with atrial fibrillation and gout had higher ischemic stroke rates, while urate-lowering therapy was associated with lower stroke rates.