To analyze the role of molecular subtypes in fertility-sparing treatment (FST) for endometrial cancer and explore the potential of immune checkpoint inhibitors (ICIs) in this context.
Approach:
Criteria for FST: Eligibility for FST includes well-differentiated endometrioid adenocarcinoma, absence of contraindications to progestin treatment, strong desire to preserve fertility, and no evidence of metastatic lesions.
Hysteroscopy: Hysteroscopic resection combined with progestin therapy is recommended for accurate pathological diagnosis and treatment, achieving higher complete remission rates compared to progestin monotherapy.
Progestin-based therapy: Medroxyprogesterone acetate (MPA) and megestrol acetate (MA) are the main progestins used, with MA showing higher remission rates. Combination therapies are also effective.
Key Findings:
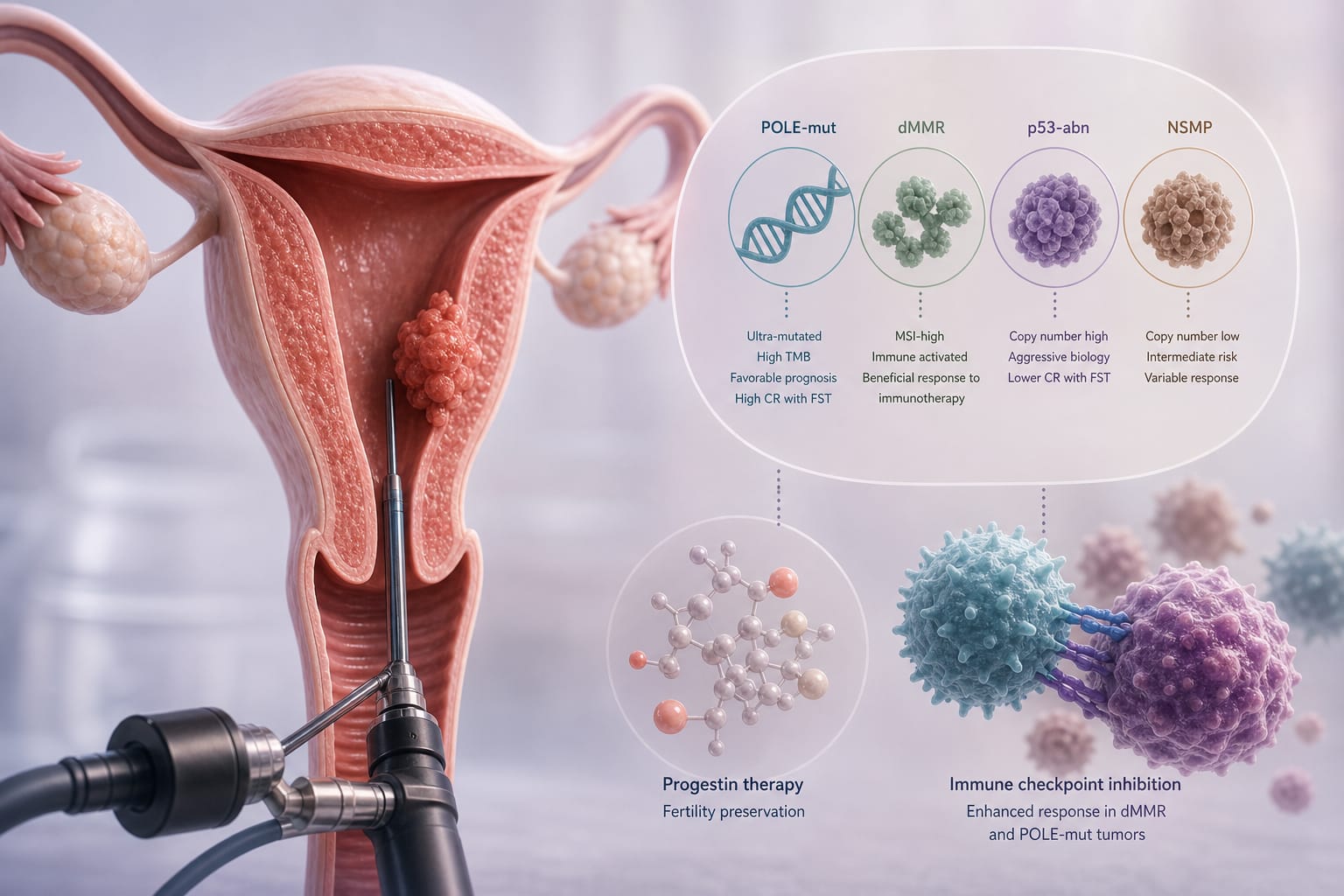
POLE mutations are associated with higher complete remission rates in fertility-sparing treatment.
Patients with dMMR endometrial cancer have a higher recurrence rate after progestin treatment.
Immune checkpoint inhibitors may play a significant role in treating dMMR patients undergoing fertility-sparing treatment.
Interpretation:
Molecular classification provides insights into prognosis and treatment strategies for endometrial cancer patients seeking fertility preservation.
Limitations:
Limited evidence exists for fertility-sparing treatment in grade 2 tumors or those with minimal myometrial invasion.
Patients with P53abn are not eligible for fertility-sparing therapy due to poor prognosis.
Conclusion:
Molecular subtyping and the potential use of ICIs represent promising avenues for improving fertility-sparing treatment outcomes in endometrial cancer.