To synthesize available evidence and identify determinants associated with thrombocytopenia in critically ill patients.
Approach:
Study Design: Systematic review and meta-analysis conducted in accordance with PRISMA guidelines.
Literature Search: Comprehensive search of multiple databases from inception to January 20, 2026, for observational studies on thrombocytopenia in ICU patients.
Eligibility Criteria: Included observational studies reporting risk factors for thrombocytopenia in critically ill patients.
Data Extraction: Data extracted independently by two reviewers, resolving disagreements through discussion.
Key Findings:
Bleeding was associated with a higher occurrence of thrombocytopenia (OR = 3.49, 95% CI: 1.70–7.19).
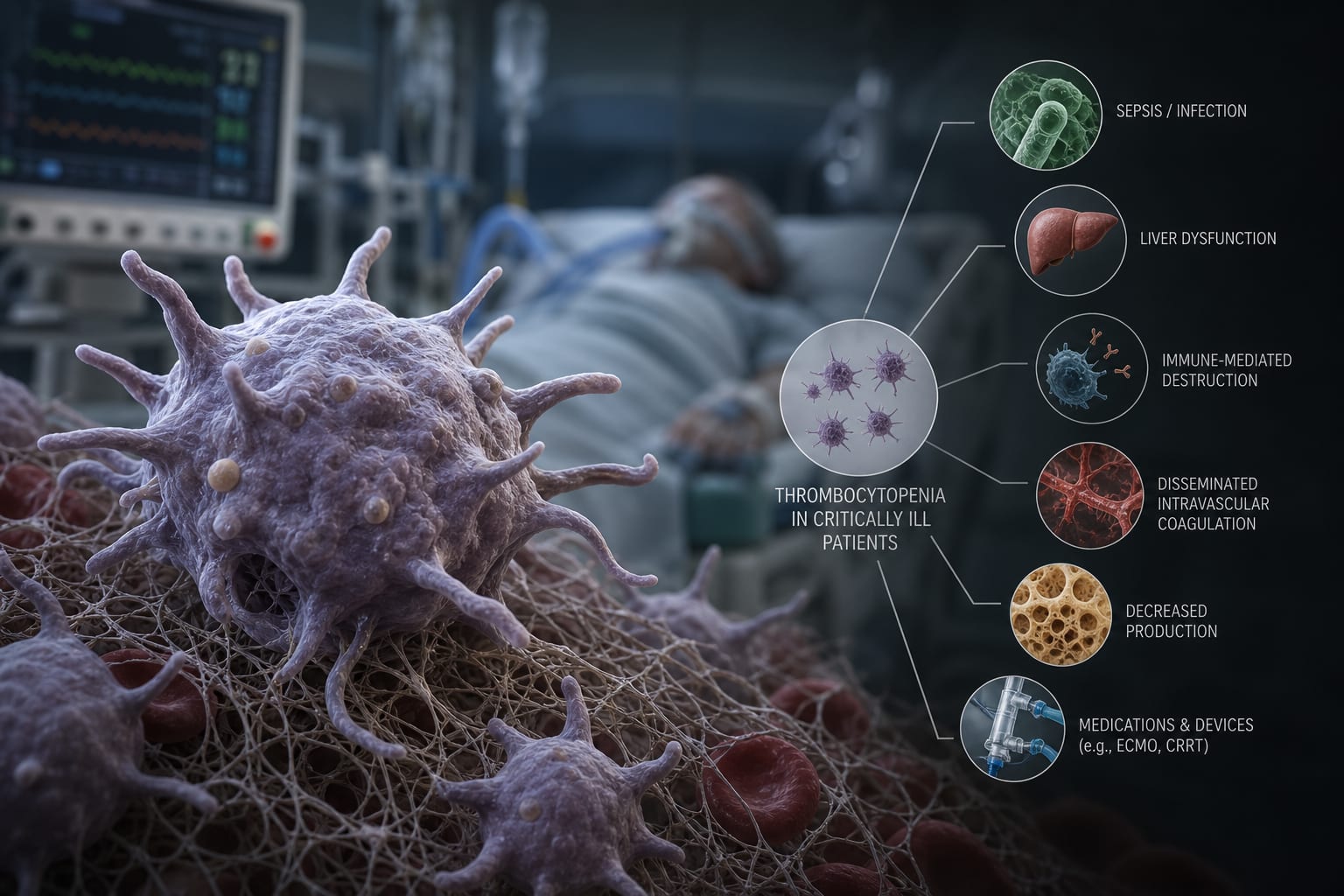
Sepsis was linked to thrombocytopenia (OR = 2.32, 95% CI: 1.74–3.09).
Impaired liver function increased the likelihood of thrombocytopenia (OR = 1.55, 95% CI: 1.14–2.11).
A Simplified Acute Physiology Score (SAPS) < 20 showed a modest association with thrombocytopenia (OR = 1.09, 95% CI: 1.05–1.14).
Interpretation:
Bleeding, sepsis, impaired liver function, and lower SAPS scores are associated with a higher likelihood of thrombocytopenia in critically ill patients.
Limitations:
Variability in patient populations and ICU settings across studies.
Differences in definitions of thrombocytopenia and statistical adjustment strategies.
Conclusion:
The findings highlight clinical conditions frequently accompanying platelet decline in ICU settings.