To present a case of a patient with ICU-acquired weakness (ICUAW) who exhibited atypical asymmetric recovery patterns due to underlying neurological complications.
Approach:
Case Presentation: A 59-year-old female with severe pneumonia and septic shock developed profound muscle weakness after acute respiratory failure. Initial diagnosis was ICUAW, but subsequent imaging revealed watershed infarctions.
Diagnostic Process: The diagnostic approach included ruling out drug-induced and metabolic factors, systemic comorbidities, and acute ICU-acquired neuromuscular complications through various tests and imaging.
Rehabilitation Strategy: A tailored rehabilitation strategy focusing on mitochondrial metabolism and active physical therapy was implemented, leading to significant functional improvement.
Key Findings:
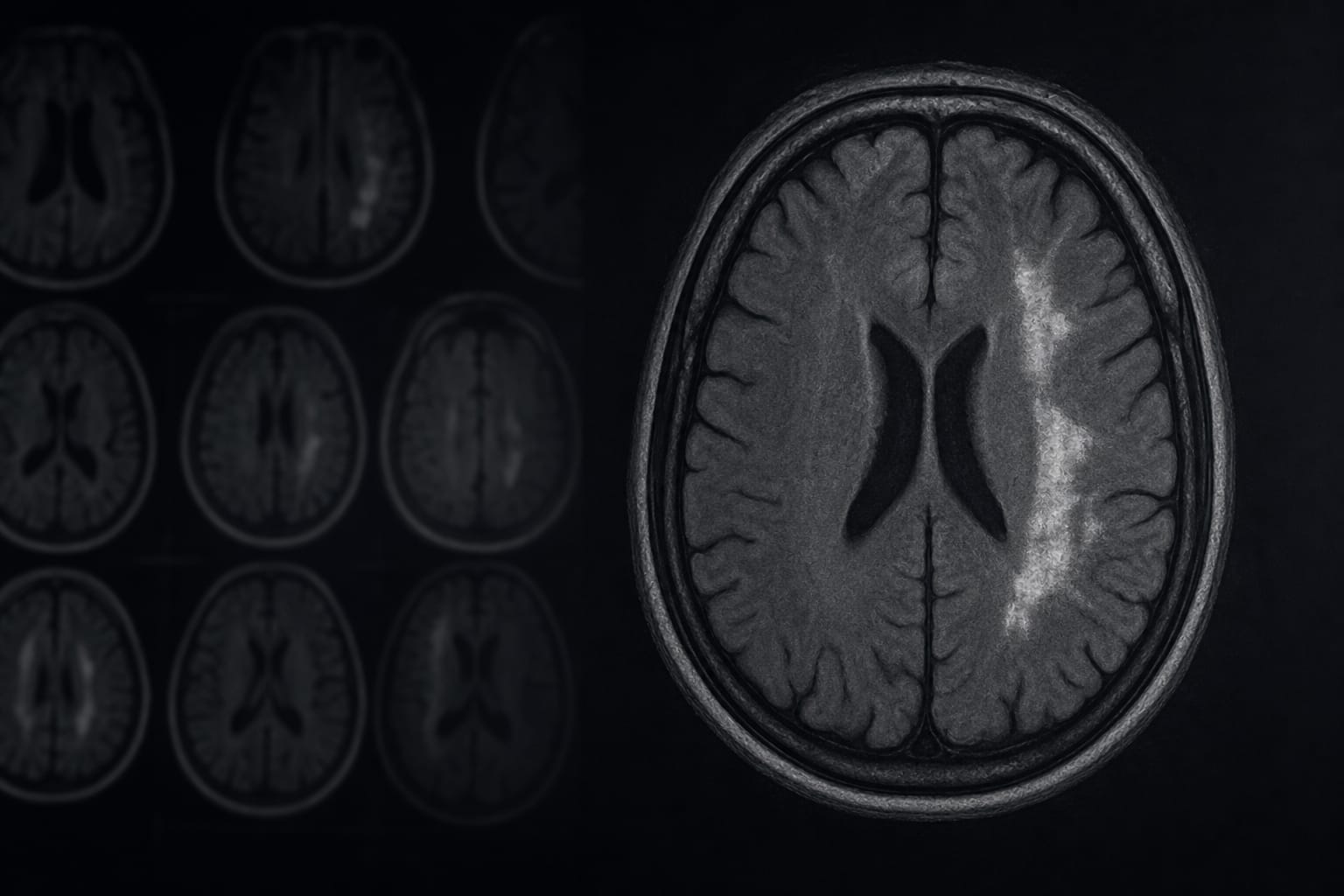
The patient exhibited distinct asymmetrical motor recovery with persistent left-sided deficits.
Cranial MRI revealed fresh watershed infarctions in the right hemisphere.
Full recovery was reported at a 2-year follow-up after a multimodal rehabilitation approach.
Interpretation:
The case illustrates that the weaning process can reveal latent cerebrovascular issues in critically ill patients, necessitating a high index of suspicion for asymmetric recovery patterns in ICUAW.
Limitations:
The case is a single patient report, limiting generalizability.
Potential confounding factors in the patient's complex medical history may complicate the interpretation of findings.
Conclusion:
Clinicians should maintain a high index of suspicion for asymmetric recovery patterns in ICUAW and consider a multimodal approach for accurate diagnosis and management.