Analysis of influencing factors and construction of nomogram prediction model for pulmonary infection in patients with acute exacerbation of chronic obstructive pulmonary disease complicated with type II respiratory failure - Summary - MDSpire
Advertisement
Analysis of influencing factors and construction of nomogram prediction model for pulmonary infection in patients with acute exacerbation of chronic obstructive pulmonary disease complicated with type II respiratory failure
To construct a risk prediction nomogram model for pulmonary infection in patients with acute exacerbation of chronic obstructive pulmonary disease (AECOPD) complicated with type II respiratory failure.
Approach:
Study Design: A retrospective analysis of clinical data from 361 patients with AECOPD and type II respiratory failure.
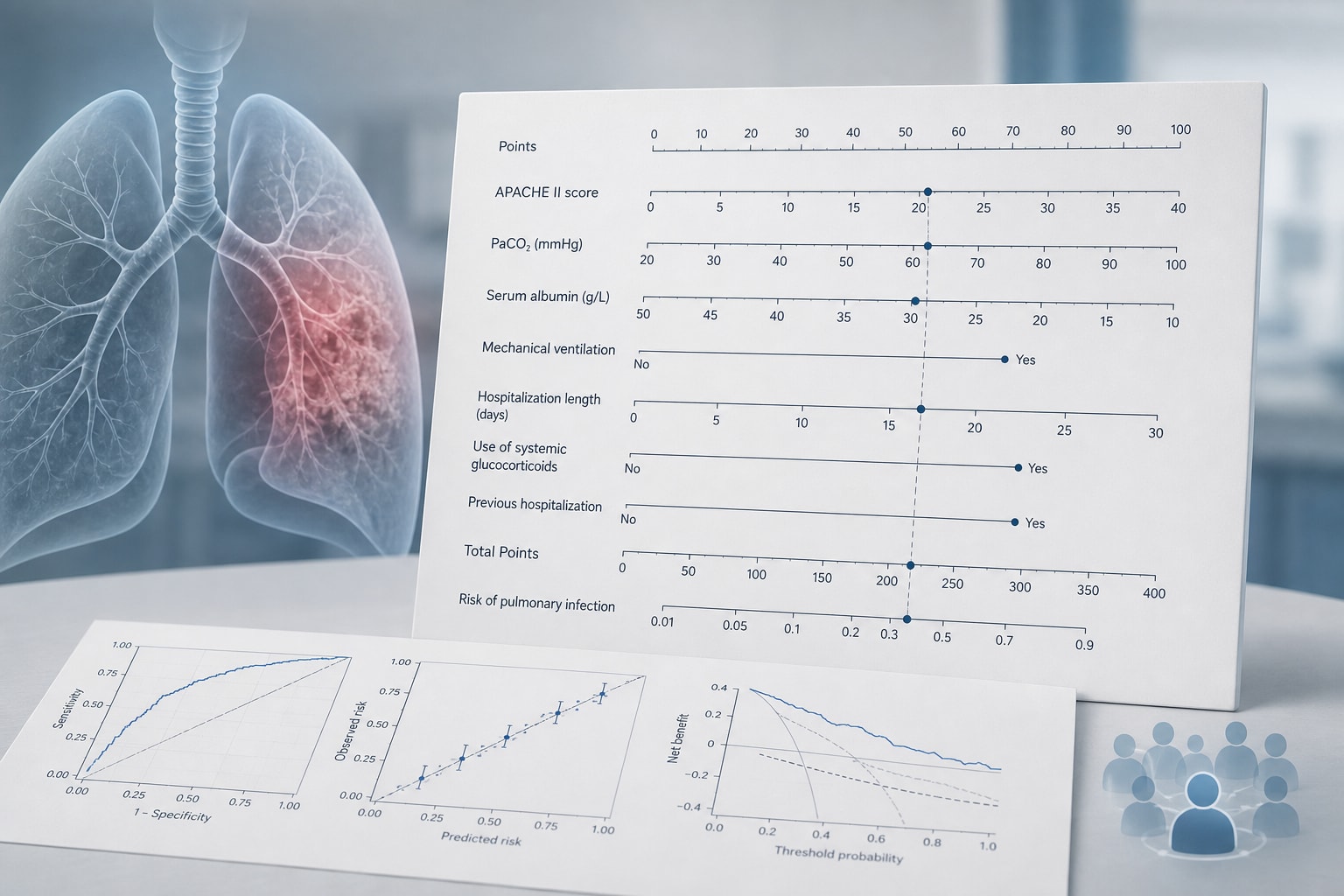
Data Analysis: Used restricted cubic spline analysis, single factor and multiple factor logistic regression analyses to identify independent risk factors and construct the predictive model.
Model Evaluation: Evaluated predictive performance using ROC curve, calibration curve, and clinical decision curve.
Key Findings:
Age showed no significant nonlinear relationship with pulmonary infection (P for nonlinearity > 0.05).
Length of hospital stay, APACHE II score, and duration of antibiotic use had significant nonlinear relationships with pulmonary infection (P for nonlinearity < 0.05).
Independent risk factors identified include age, diabetes, hospital stay > 15 days, APACHE II score > 15 points, and antibiotics combination time > 14 days.
Albumin was identified as an independent protective factor (P < 0.05).
The nomogram model demonstrated AUCs of 0.917 and 0.884 in training and validation cohorts, respectively.
Interpretation:
The nomogram model may assist in identifying pulmonary infection risk in AECOPD patients with type II respiratory failure.
Limitations:
Retrospective design may introduce bias.
Single-center study limits generalizability.
Conclusion:
The constructed nomogram risk model may demonstrate predictive performance for pulmonary infection in AECOPD patients with type II respiratory failure.