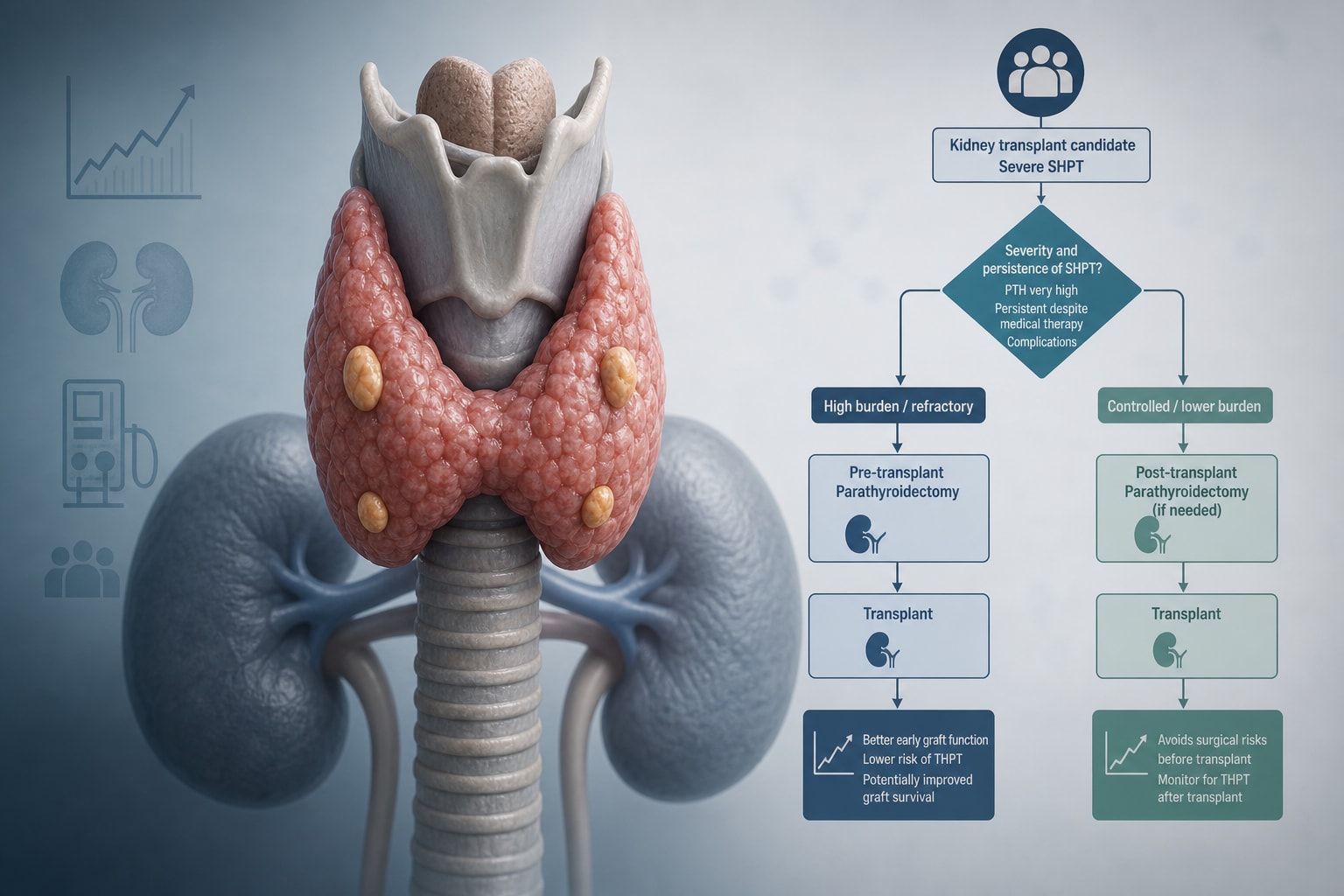
To compare the outcomes of pre-transplant PTx and post-transplant PTx on graft loss, tertiary hyperparathyroidism (THPT), renal function, and complications, and to propose a clinical algorithm for PTx timing based on these outcomes.
Approach:
Method: A
Method: s
Method: y
Method: s
Method: t
Method: e
Method: m
Method: a
Method: t
Method: i
Method: c
Method: s
Method: e
Method: a
Method: r
Method: c
Method: h
Method: o
Method: f
Method: P
Method: u
Method: b
Method: M
Method: e
Method: d
Method: ,
Method: E
Method: m
Method: b
Method: a
Method: s
Method: e
Method: ,
Method: W
Method: e
Method: b
Method: o
Method: f
Method: S
Method: c
Method: i
Method: e
Method: n
Method: c
Method: e
Method: ,
Method: a
Method: n
Method: d
Method: C
Method: o
Method: c
Method: h
Method: r
Method: a
Method: n
Method: e
Method: L
Method: i
Method: b
Method: r
Method: a
Method: r
Method: y
Method: w
Method: a
Method: s
Method: c
Method: o
Method: n
Method: d
Method: u
Method: c
Method: t
Method: e
Method: d
Method: f
Method: r
Method: o
Method: m
Method: i
Method: n
Method: c
Method: e
Method: p
Method: t
Method: i
Method: o
Method: n
Method: t
Method: o
Method: J
Method: u
Method: l
Method: y
Method: 2
Method: 0
Method: 2
Method: 4
Method: ,
Method: w
Method: i
Method: t
Method: h
Method: a
Method: n
Method: u
Method: p
Method: d
Method: a
Method: t
Method: e
Method: i
Method: n
Method: A
Method: p
Method: r
Method: i
Method: l
Method: 2
Method: 0
Method: 2
Method: 6
Method: ,
Method: t
Method: o
Method: i
Method: d
Method: e
Method: n
Method: t
Method: i
Method: f
Method: y
Method: s
Method: t
Method: u
Method: d
Method: i
Method: e
Method: s
Method: c
Method: o
Method: m
Method: p
Method: a
Method: r
Method: i
Method: n
Method: g
Method: p
Method: r
Method: e
Method: -
Method: t
Method: r
Method: a
Method: n
Method: s
Method: p
Method: l
Method: a
Method: n
Method: t
Method: a
Method: n
Method: d
Method: p
Method: o
Method: s
Method: t
Method: -
Method: t
Method: r
Method: a
Method: n
Method: s
Method: p
Method: l
Method: a
Method: n
Method: t
Method: P
Method: T
Method: x
Method: i
Method: n
Method: a
Method: d
Method: u
Method: l
Method: t
Method: k
Method: i
Method: d
Method: n
Method: e
Method: y
Method: t
Method: r
Method: a
Method: n
Method: s
Method: p
Method: l
Method: a
Method: n
Method: t
Method: c
Method: a
Method: n
Method: d
Method: i
Method: d
Method: a
Method: t
Method: e
Method: s
Method: .
Key Findings:
Eight studies involving 4355 patients were included.
Graft loss events were low in both groups, with a trend toward lower graft loss in the pre-transplant PTx group; one study reported a significant adjusted odds ratio favoring pre-transplant PTx (0.547, 95% CI: 0.327–0.913).
Pre-transplant PTx was associated with lower 1-month eGFR but no long-term differences in eGFR or serum creatinine were observed.
Postoperative hypocalcemia rates were inconsistent across studies.
A large database study indicated higher 30-day composite morbidity for pre-transplant PTx without differences in mortality.
Interpretation:
Pre-transplant PTx may be associated with lower graft loss and comparable long-term renal function compared to post-transplant PTx. A personalized approach using a proposed algorithm may optimize clinical decision-making.
Limitations:
All included studies were observational, limiting the strength of the evidence.
Heterogeneity in outcome definitions and measurement methods prevented meta-analysis.
No relevant interventional studies have been published to date.
Conclusion:
A risk-stratified algorithm is proposed to guide PTx timing. Prospective studies are needed to validate this framework.