To propose a UA–kidney–immune–vascular framework for understanding accelerated coronary artery calcification (CAC) in diabetic kidney disease (DKD), emphasizing the need for a broader mechanistic understanding.
Key Findings:
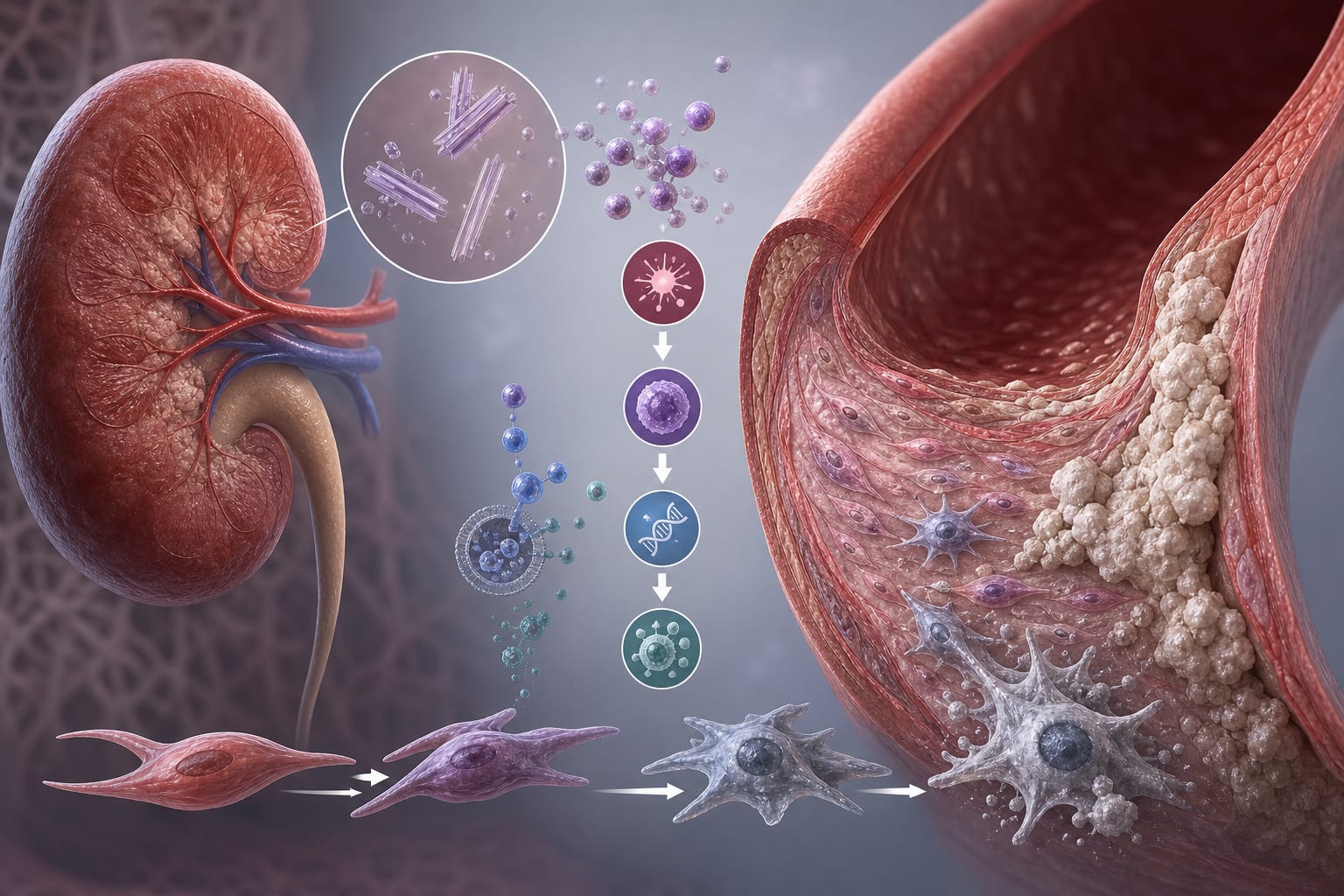
CAC progresses rapidly in patients with DKD and is associated with hyperuricemia.
Elevated UA may contribute to oxidative stress and inflammation, affecting vascular smooth muscle cells and endothelial function, though causation is not established.
Emerging studies suggest kidney-derived signals may propagate inflammation to vascular tissues.
Interpretation:
The framework emphasizes evidence-supported mechanisms and emerging concepts, while acknowledging that UA is not established as an isolated causal determinant of CAC.
Limitations:
Direct evidence from DKD kidney tissue regarding UA's role is limited, which may affect the interpretation of findings.
Current understanding is largely based on extrapolated data from hyperuricemia or high-fructose models, necessitating caution in generalization.
Conclusion:
The review organizes existing evidence to guide future research on the relationship between UA and CAC in DKD, without asserting it as a definitive model.