To synthesize six inter-related paradigm shifts in the understanding of preeclampsia, challenging the prevailing two-stage model of placental pathophysiology.
Approach:
Key Findings:
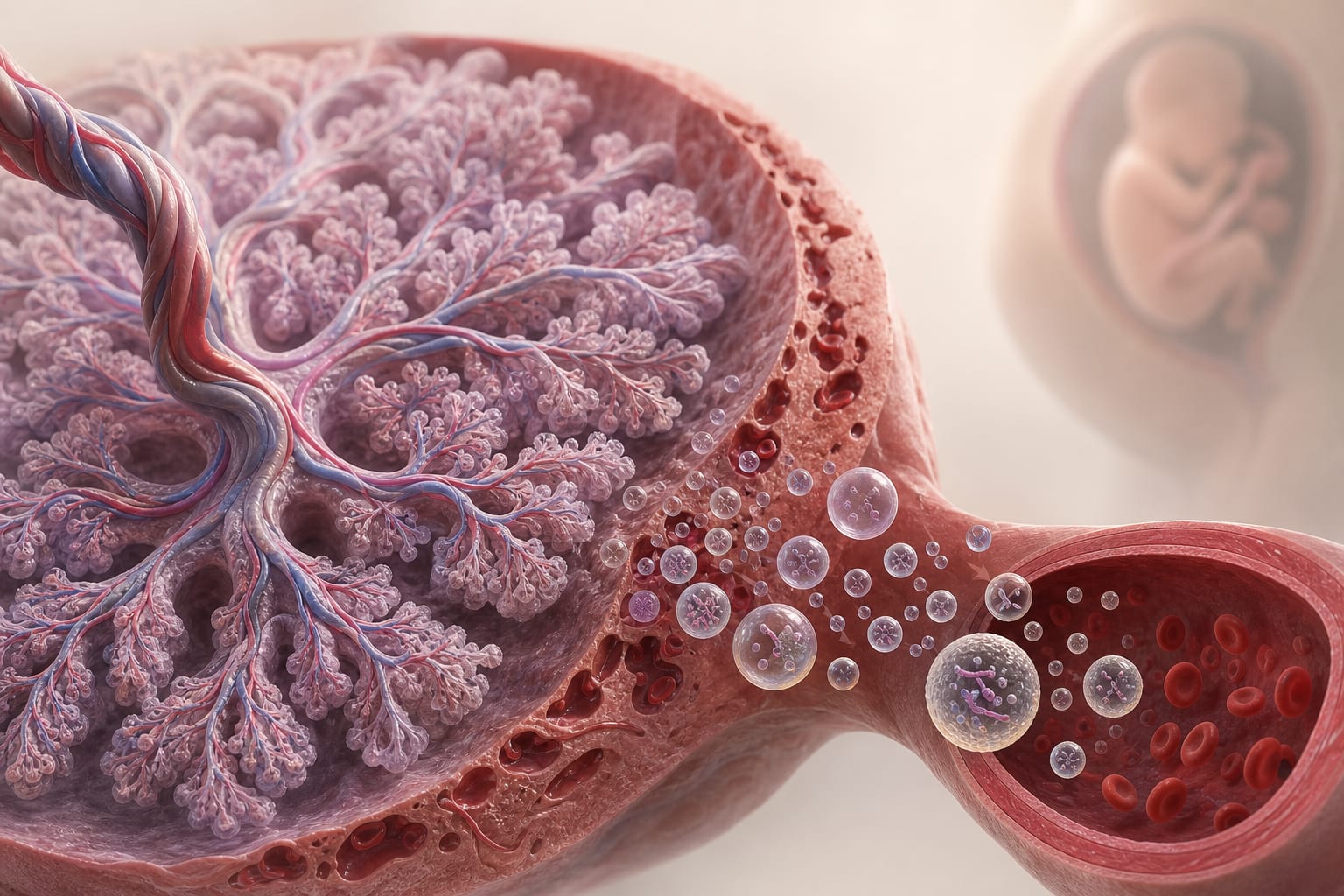
First-trimester villous origins are critical rather than second-trimester deep-placentation failure.
Intervillous hyperoxia is observed in early-onset disease instead of placental hypoxia.
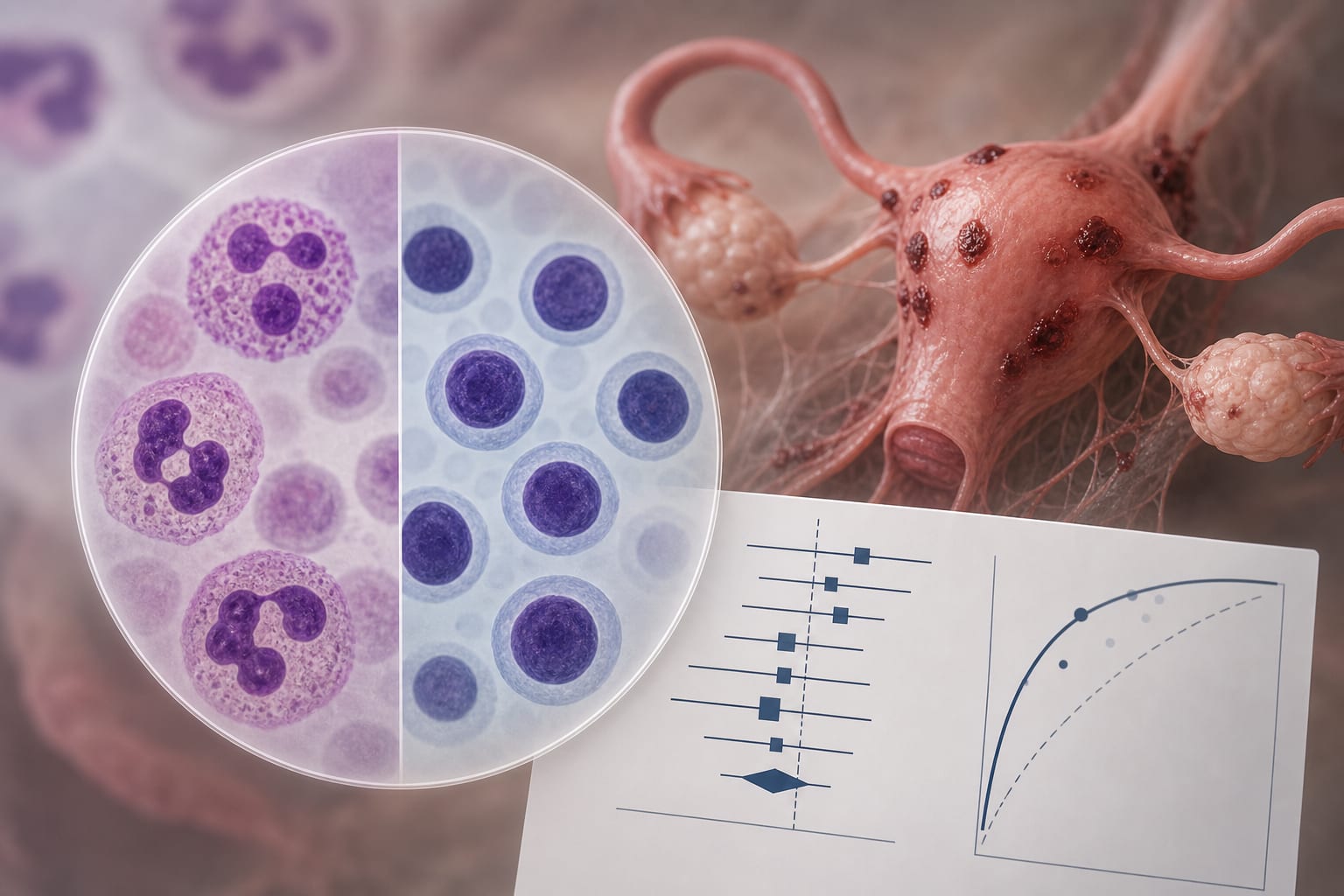
Metabolic and glycocalyx-based pathogenesis is more relevant than pure angiogenic imbalance.
The placenta functions as an endogenous exposome via extracellular vesicles.
Steroid imbalance and alternative renin–angiotensin–leptin signaling are significant.
Reduced immune tolerance and dynamic in vitro models challenge previous static interpretations.
Interpretation:
These shifts suggest a redefinition of preeclampsia as a first-trimester syndrome linked to villous trophoblast dysregulation, impacting maternal endothelial health through various pathways.
Limitations:
Several propositions require independent replication in cohorts beyond the originating research environment.
The shifts do not individually overturn the two-stage framework but collectively suggest a need for broader assessment strategies.
Conclusion:
The findings advocate for earlier, multimodal risk assessment and biomarker panels in maternal-fetal medicine, extending beyond current practices.
A JAMA Internal Medicine Viewpoint urges clinicians and health systems to verify risk-model inputs before acting on automated breast cancer screening recommendations.