Prognostic significance of interstitial fibrosis and tubular atrophy in biopsy-proven diabetic kidney disease: a single-center retrospective cohort study - Summary - MDSpire
Advertisement
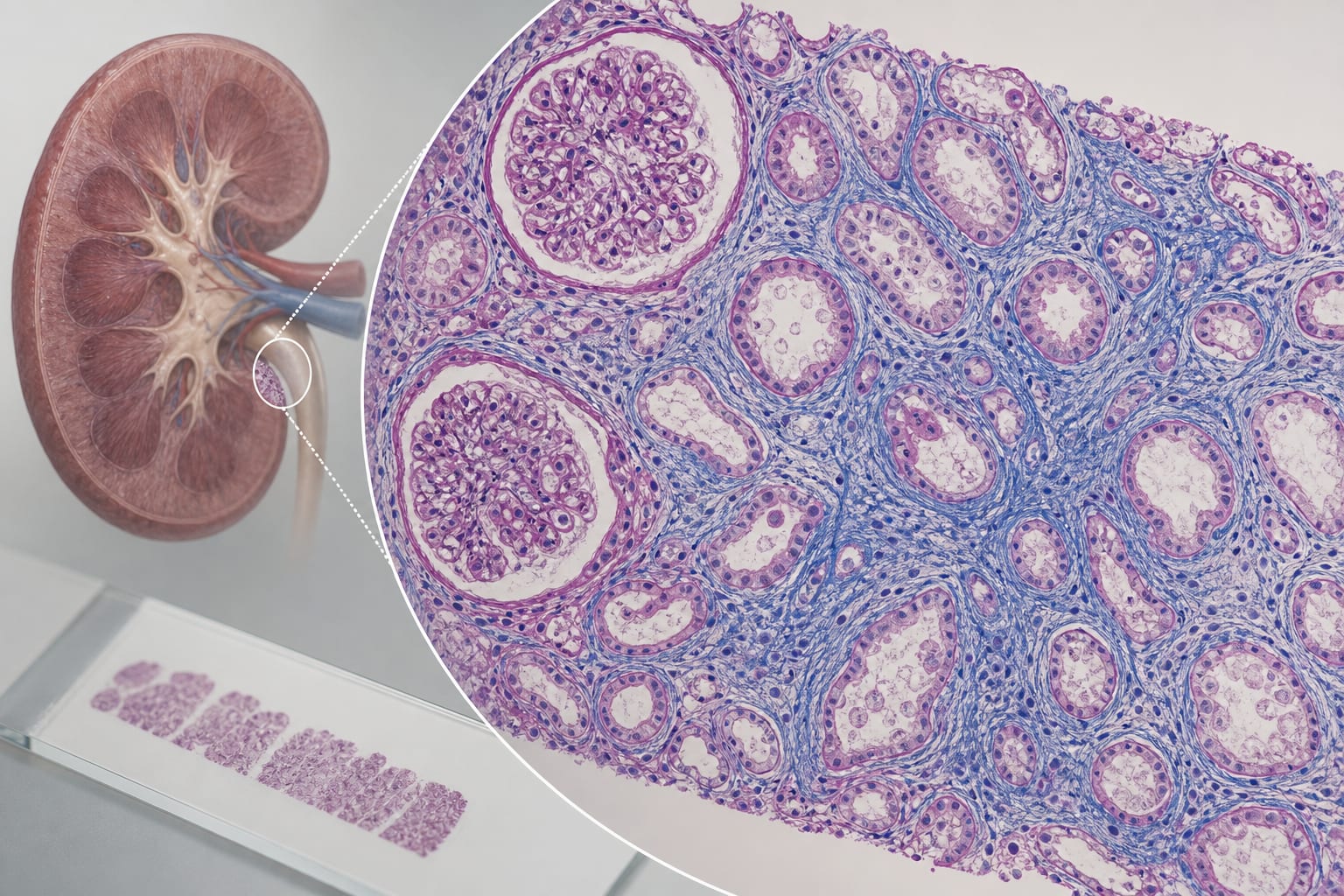
Prognostic significance of interstitial fibrosis and tubular atrophy in biopsy-proven diabetic kidney disease: a single-center retrospective cohort study
To evaluate the association between interstitial fibrosis and tubular atrophy (IFTA) severity and kidney outcomes in patients with biopsy-proven diabetic kidney disease (DKD).
Approach:
Study Design: Retrospective cohort study of 164 patients with type 2 diabetes and biopsy-confirmed pure DKD, followed for a median of 38 months.
Outcome Measures: Primary composite kidney endpoint was initiation of kidney replacement therapy or kidney-related death.
Statistical Analysis: LASSO Cox regression and random survival forest were used to identify predictors of kidney outcomes.
Key Findings:
34 patients reached the composite kidney endpoint.
IFTA score 2/3 was associated with a higher risk of the composite kidney endpoint (HR 3.96, 95% CI 1.71–9.16, P = 0.001).
Higher 24-hour proteinuria (HR 1.52, 95% CI 1.19–1.94, P < 0.001) and lower serum calcium (HR 0.140, 95% CI 0.041–0.481, P = 0.002) were also independently associated with poor kidney outcomes.
Patients with IFTA 2/3 had significantly lower kidney survival compared to those with IFTA 1 (log-rank P = 0.0056).
Interpretation:
IFTA severity, along with proteinuria and serum calcium levels, are important prognostic factors in biopsy-proven DKD.
Limitations:
Retrospective design may introduce selection bias.
Single-center study limits generalizability of findings.
Further studies are needed to confirm these findings.
Conclusion:
IFTA 2/3 is associated with adverse kidney outcomes in biopsy-proven DKD.