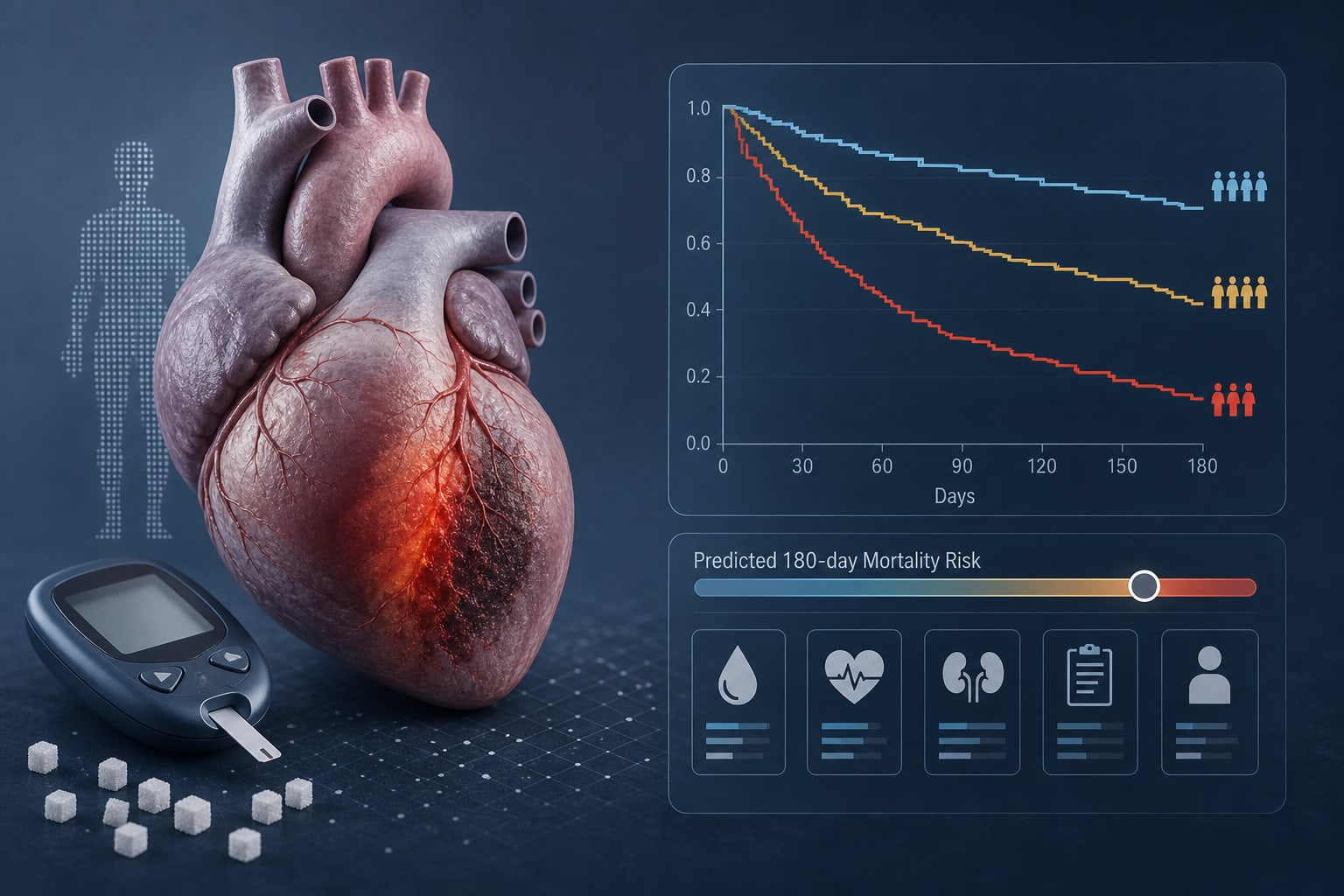
To assess admission risk heterogeneity in patients with diabetic acute myocardial infarction (DM-AMI) and develop a model for predicting 180-day mortality using routine variables.
Approach:
Study Design: Retrospective dual-cohort study including AMI patients from a Beijing tertiary hospital (development cohort) and an ICU-based MIMIC-IV cohort (external validation).
Model Development: A Cox model was built using admission variables to predict 180-day mortality.
Model Evaluation: Model performance was evaluated using discrimination, calibration, and decision curve analysis with internal bootstrap validation and comparison with GRACE.
Key Findings:
Among 4,167 patients, 1,514 had DM-AMI with 90 deaths at 180 days.
The model included eight variables: age, heart rate, SBP, glucose, BUN, hemoglobin, RDW, WBC.
The model showed good discrimination in the development cohort (C-index 0.848; AUC 0.857) and maintained performance externally (AUC 0.744).
The combined model improved performance compared to GRACE (ΔAUC = 0.014, P = 0.031).
Calibration in MIMIC-IV indicated risk overestimation (slope 0.527; O/E 0.652).
Interpretation:
DM-AMI patients exhibit marked admission risk heterogeneity. The model provides prognostic information beyond GRACE but requires recalibration for use in external settings.
Limitations:
The model requires recalibration for accurate risk assessment in external cohorts.
Risk overestimation was noted in the external validation cohort.
Conclusion:
The model developed offers a parsimonious approach to predict 180-day mortality in DM-AMI patients.
An interpretable machine-learning model classified angiographic coronary artery disease in patients referred for coronary angiography, but high disease prevalence and unclear inflammatory signals limited clinical interpretation.