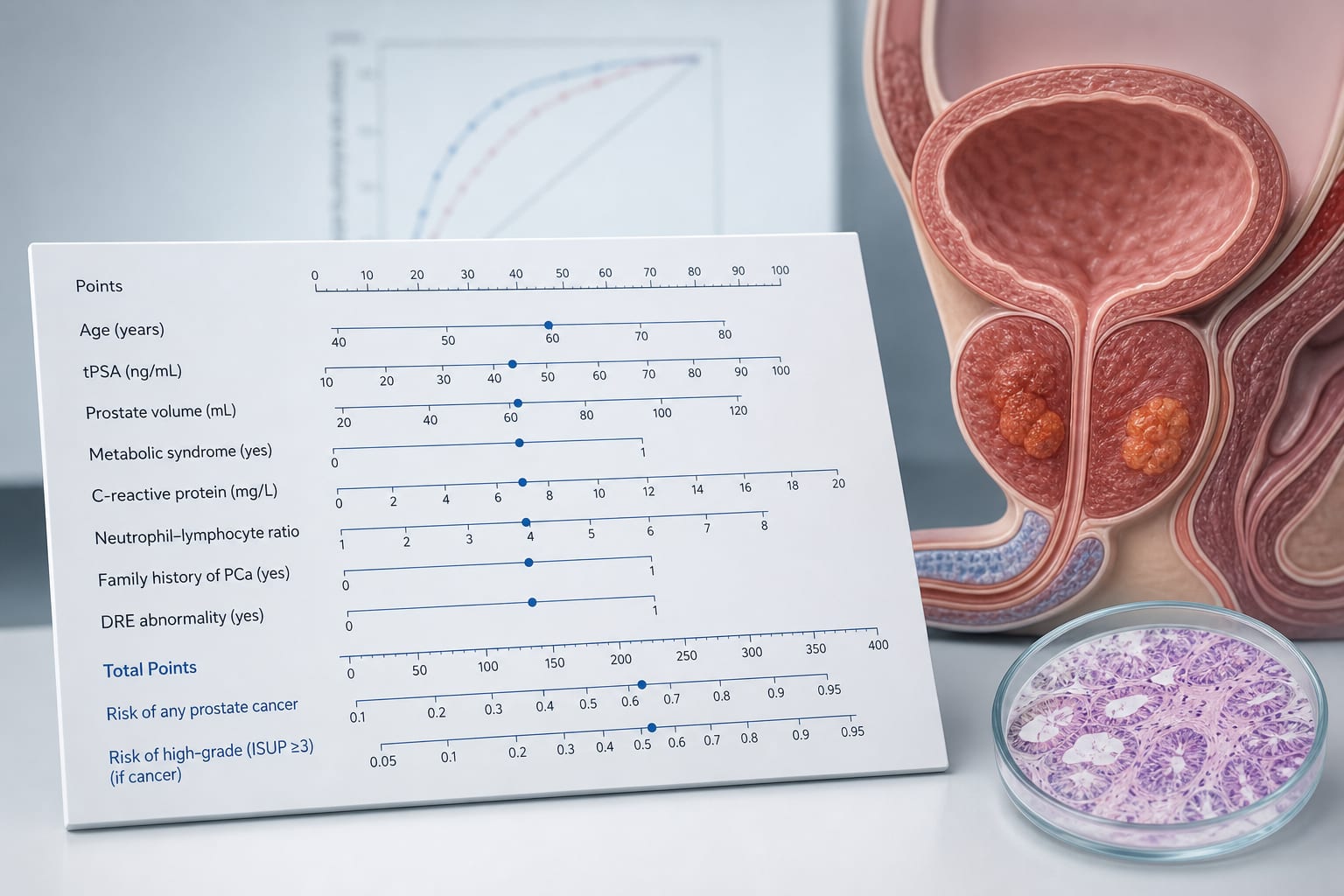
To develop a model integrating multidimensional indicators, including metabolic and inflammatory factors, to predict prostate cancer and high−grade disease in men with tPSA >10 ng/mL.
Approach:
Study Design: Retrospective study including 461 men who underwent prostate biopsy with tPSA >10 ng/mL, split into training (70%) and validation (30%) sets.
Model Development: Two logistic regression models were built: Model 1 for benign vs. malignant and Model 2 for high−grade vs. low−grade malignant cases.
Variable Selection: Variables with VIF>5 were excluded; backward stepwise selection and univariate P < 0.05 guided variable selection.
Performance Assessment: Model performance was assessed using AUC, calibration, DCA, and compared with fPSA% alone using DeLong test.
Key Findings:
54.7% of patients had prostate cancer, and 55.2% of malignant cases were classified as high−grade based on ISUP criteria.
Malignant patients had higher BMI, TyG index, NLR, and tPSA, and lower fPSA% (all P < 0.05).
Model 1 AUC was 0.871; Model 2 AUC was 0.779.
Optimal thresholds yielded sensitivity/specificity of 80.3%/74.6% (Model 1) and 71.7%/62.1% (Model 2).
Both models showed good calibration (Hosmer−Lemeshow P>0.05) and higher net benefit than fPSA% alone (P < 0.05).
Interpretation:
Two nomograms using routine clinical and laboratory variables may assist in risk stratification for prostate cancer and high−grade disease in men with tPSA >10 ng/mL.
Limitations:
Single-center study may limit generalizability and the applicability of the findings.
Retrospective design may introduce selection bias.
Conclusion:
The developed nomograms can help reduce unnecessary biopsies.