To analyze the incidence, risk factors, and outcomes of Pneumocystis jirovecii pneumonia (PJP) in immunocompromised individuals, particularly focusing on cancer-related immunosuppression, highlighting the increasing prevalence of PJP in these populations.
Key Findings:
Out of 922,200 individuals, 152 patients had 171 PJP episodes, with a hospitalization rate of 88.3% specific to these episodes and a 30-day mortality rate of 24.5%.
Hematologic malignancies were the most common immunosuppressive condition associated with PJP (42.6%).
HIV infection was present in 13.9% of PJP episodes, but no deaths occurred within 30 days in HIV-positive individuals.
Rheumatic diseases had the highest risk for contracting PJP (HR 4.01), while solid malignancies had the highest risk for mortality (HR 4.68).
Immunocompromised individuals had a significantly higher risk of hospitalization (HR 49.87) and death (HR 54.84).
Interpretation:
Immunosuppression is the primary risk factor for PJP, with specific conditions like hematologic malignancies and high-dose systemic steroids significantly affecting outcomes, underscoring the need for targeted clinical interventions.
Limitations:
Lack of validation of PJP diagnoses through microbiological testing.
Reliance on coded medical information may introduce misclassification bias, potentially affecting the accuracy of the findings.
Conclusion:
PJP remains a significant health threat in immunocompromised patients, particularly those with hematologic malignancies and on high-dose steroids, highlighting the need for vigilant monitoring and management strategies for at-risk populations.
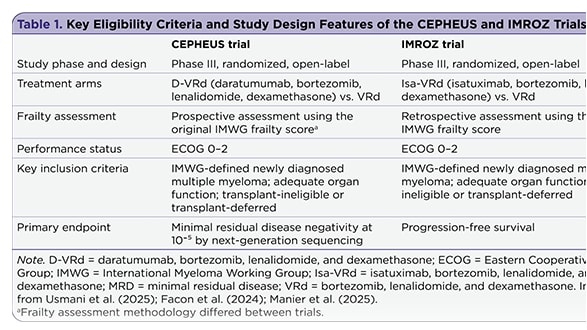
The management of newly diagnosed transplant-ineligible multiple myeloma remains challenging, in part due to the complexity of treatment decisions for frail patients. Recent subgroup analyses provide insight into whether quadruplet therapy may offer advantages over triplet therapy in this population.