To summarize the cellular and molecular mechanisms underlying immune suppression in glioblastoma (GBM) and discuss emerging therapeutic strategies aimed at overcoming these barriers.
Approach:
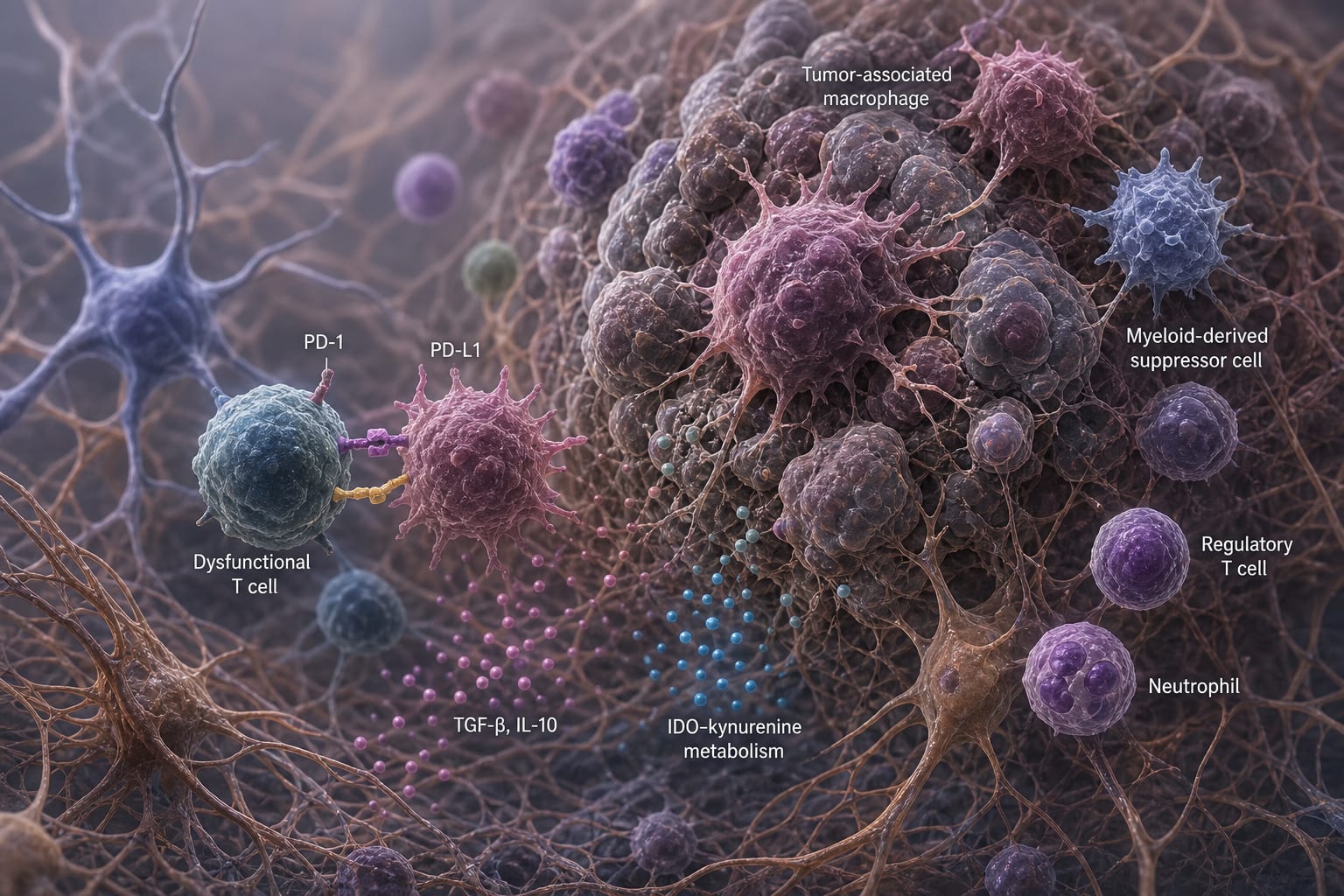
Overview of GBM: GBM is characterized by a profoundly immunosuppressive tumor microenvironment that limits effective antitumor immunity, including immune exclusion and T-cell dysfunction.
Mechanisms of Immune Suppression: The review details the roles of tumor-associated macrophages, microglia, myeloid-derived suppressor cells, and other immune cells in establishing a suppressive niche through various mechanisms.
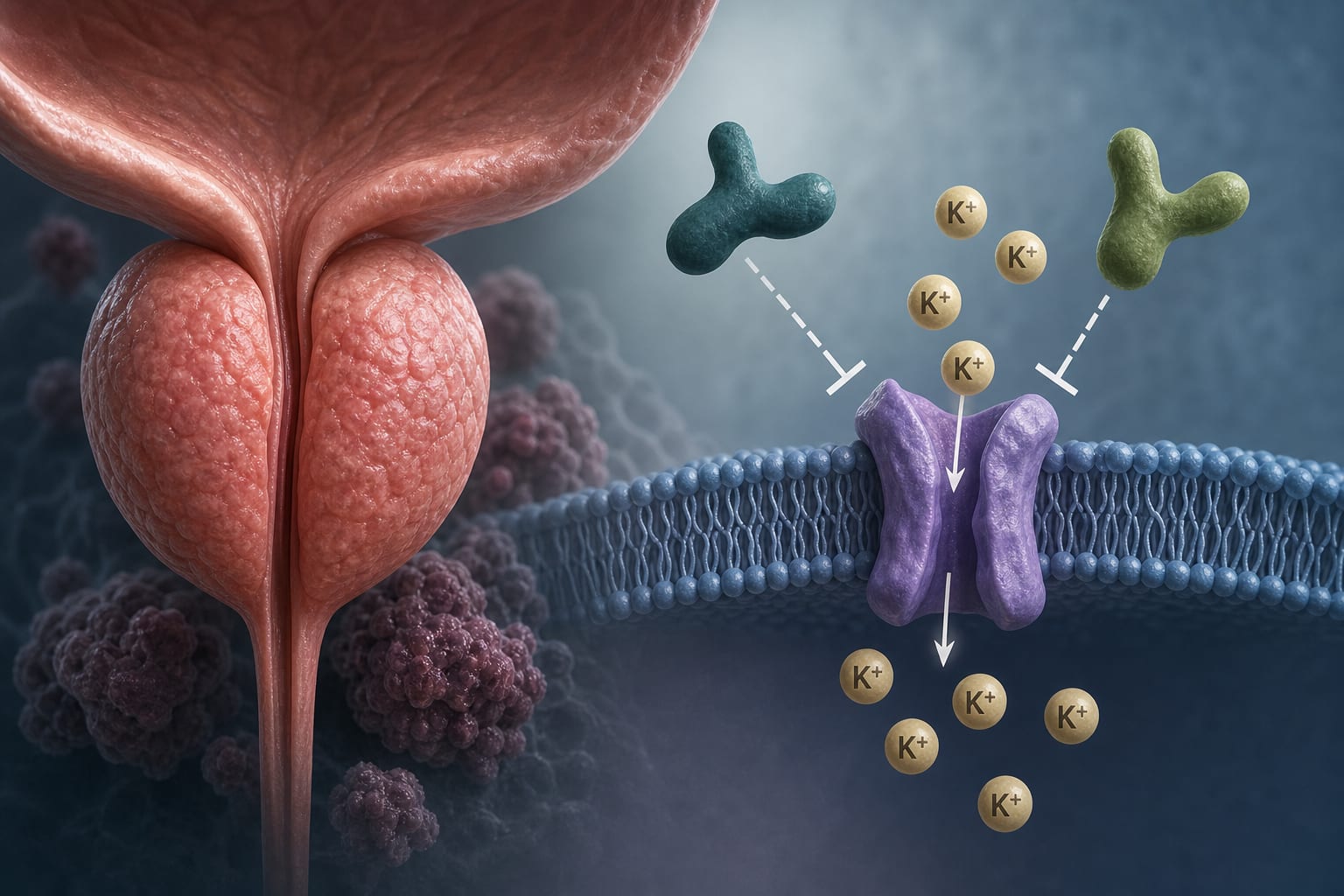
Key Pathways: Key pathways such as TGF-β/SMAD, IL-10/STAT3, IDO–kynurenine metabolism, and others are discussed for their roles in maintaining immune evasion.
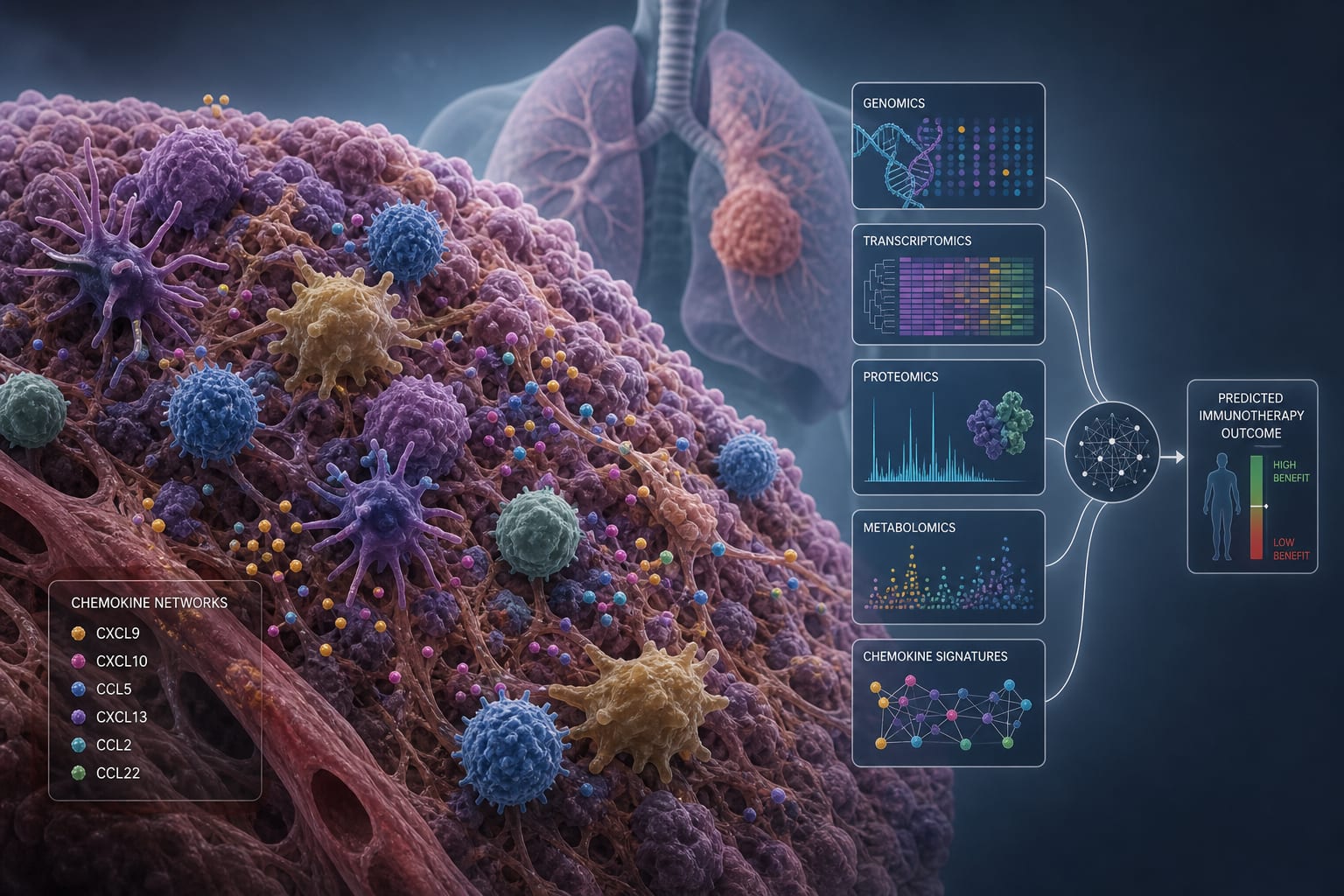
Emerging Therapeutic Strategies: The article discusses potential strategies including myeloid reprogramming, checkpoint blockade, and metabolic interventions, among others.
Key Findings:
GBM has a profoundly immunosuppressive microenvironment characterized by immune exclusion and T-cell dysfunction.
Tumor-associated macrophages and microglia play crucial roles in orchestrating immune suppression.
Key signaling pathways contribute to the maintenance of immune evasion in GBM.
Single-agent immunotherapy has rarely achieved durable benefits in GBM due to the complex immune landscape.
Interpretation:
A comprehensive understanding of GBM's immunosuppressive mechanisms is essential for developing effective combination therapies.
Limitations:
The review does not provide specific clinical trial data to support the discussed therapeutic strategies.
The complexity of GBM's immune microenvironment may limit the generalizability of proposed interventions.
Conclusion:
Understanding the interconnected barriers in GBM may guide the development of multimodal strategies to enhance therapeutic responses.
Data highlights limitations of ctDNA assay used to predict outcomes in participants with renal cell carcinoma treated with adjuvant pembrolizumab in the KEYNOTE-564 trial. Dana-Farber Cancer Institute's Dr. Toni Choueiri explains that ctDNA+ was associated with worse disease-free outcomes, but sensitivity was low.