To develop a clinically interpretable machine learning system for early-stage AKI risk assessment in critically ill pediatric patients.
Approach:
Data Handling: The dataset was divided into training (70%) and validation (30%) sets; LASSO regression was used for feature selection to enhance model performance, and the Boruta algorithm was employed to identify important features.
Key Findings:
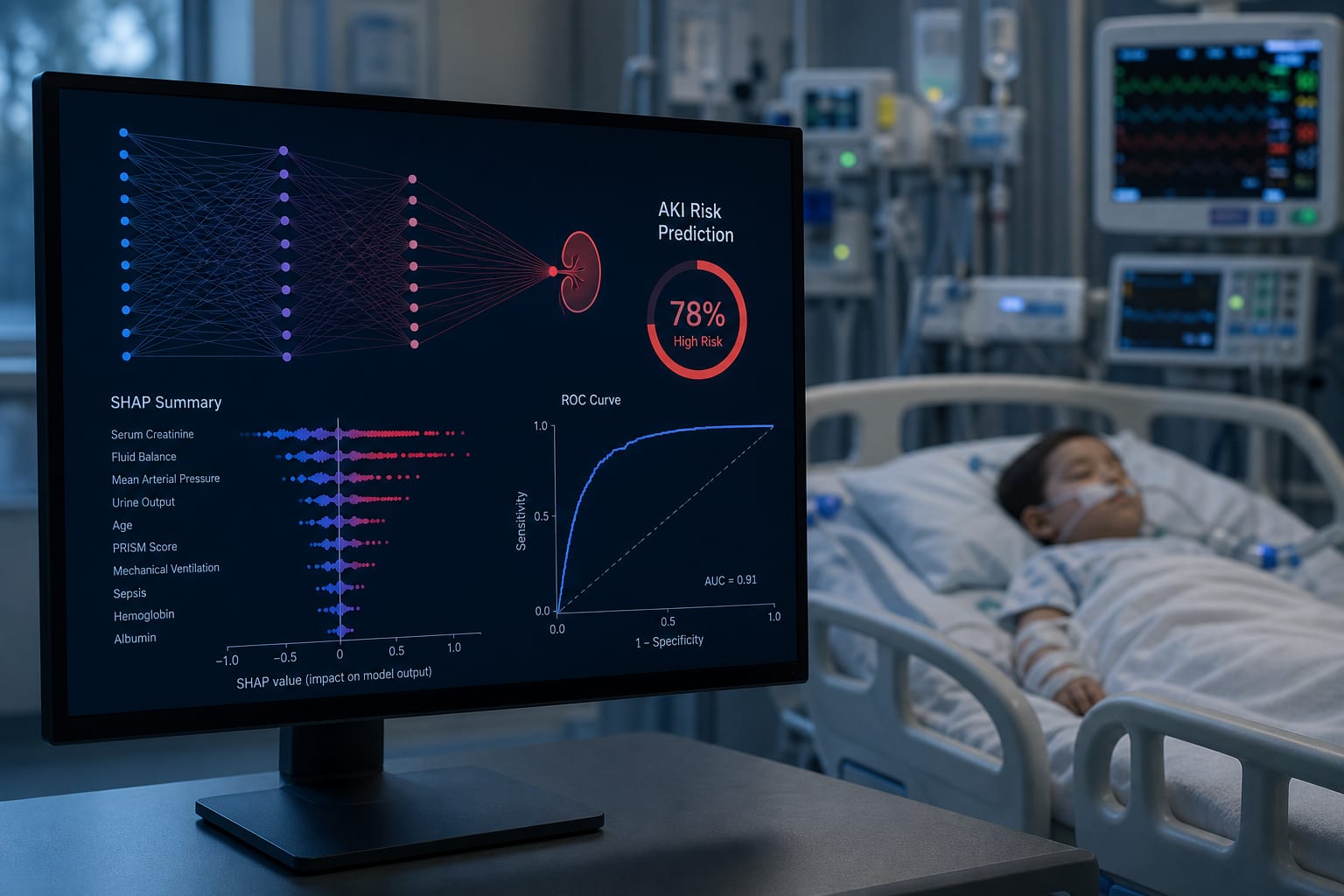
The XGBoost model showed the best risk stratification performance on the validation set.
SHAP analysis identified bicarbonate, magnesium, activated partial thromboplastin time, lymphocyte count, and thrombin time as key predictive features.
Interpretation:
The developed AKI risk stratification model demonstrated acceptable discriminative ability and clinical interpretability, potentially aiding early intervention.
Limitations:
The study is retrospective and based on a single-center database.
Generalizability to other populations may be limited.
Conclusion:
The study successfully developed a machine learning model for early AKI risk prediction in critically ill children, emphasizing model interpretability.