To summarize the anatomy, angioarchitecture, natural history, classification, treatment strategies, complications, and outcomes of craniocervical junction arteriovenous fistulas (AVFs).
Approach:
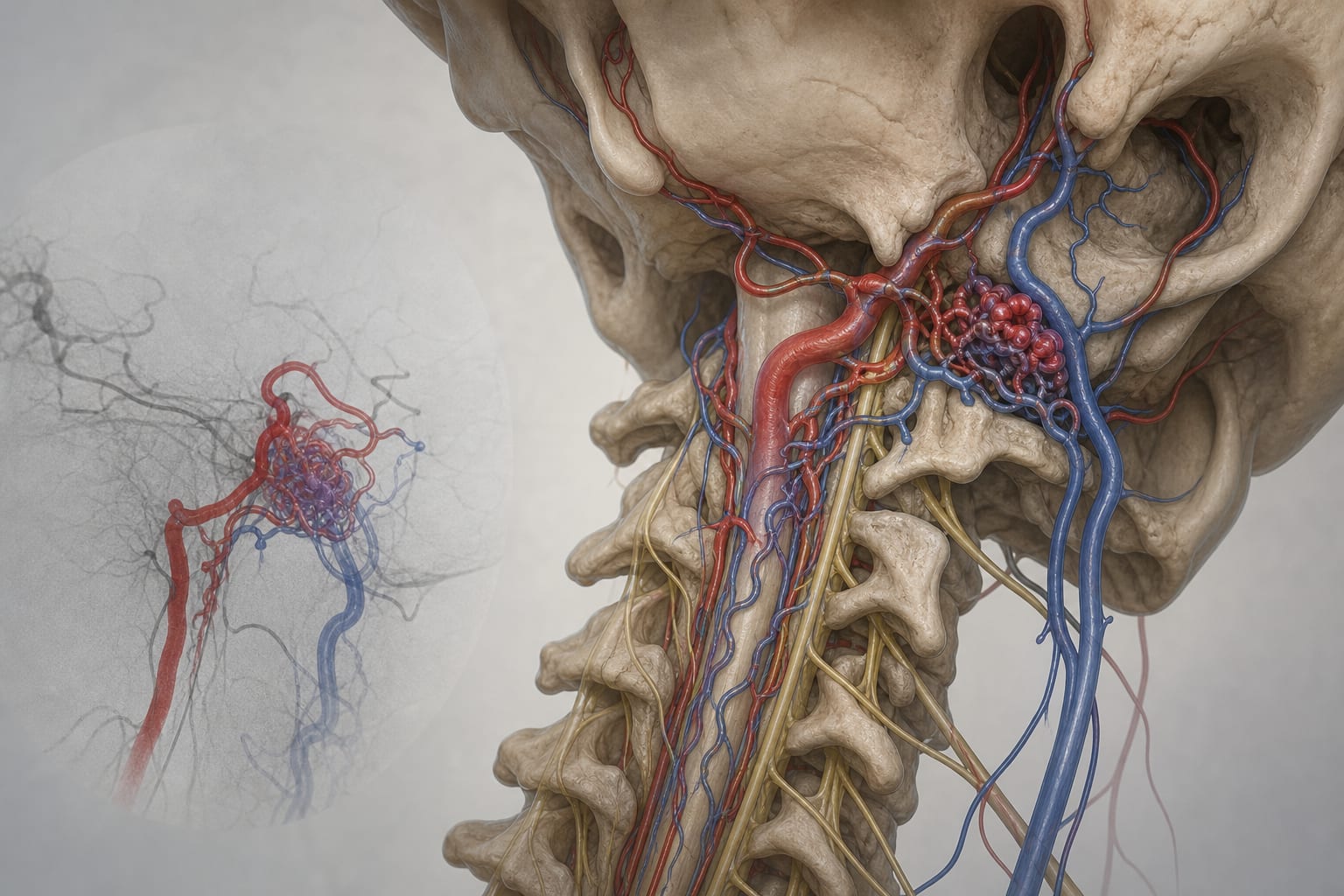
Anatomy and Angioarchitecture: Describes the complex anatomical structure of the craniocervical junction (CCJ) and the unique angioarchitecture of CCJ AVFs, including arterial feeders and venous drainage patterns.
Natural History: Discusses the clinical presentations of CCJ AVFs, primarily subarachnoid hemorrhage (SAH) and venous hypertensive myelopathy (VHM), and their correlation with venous drainage patterns.
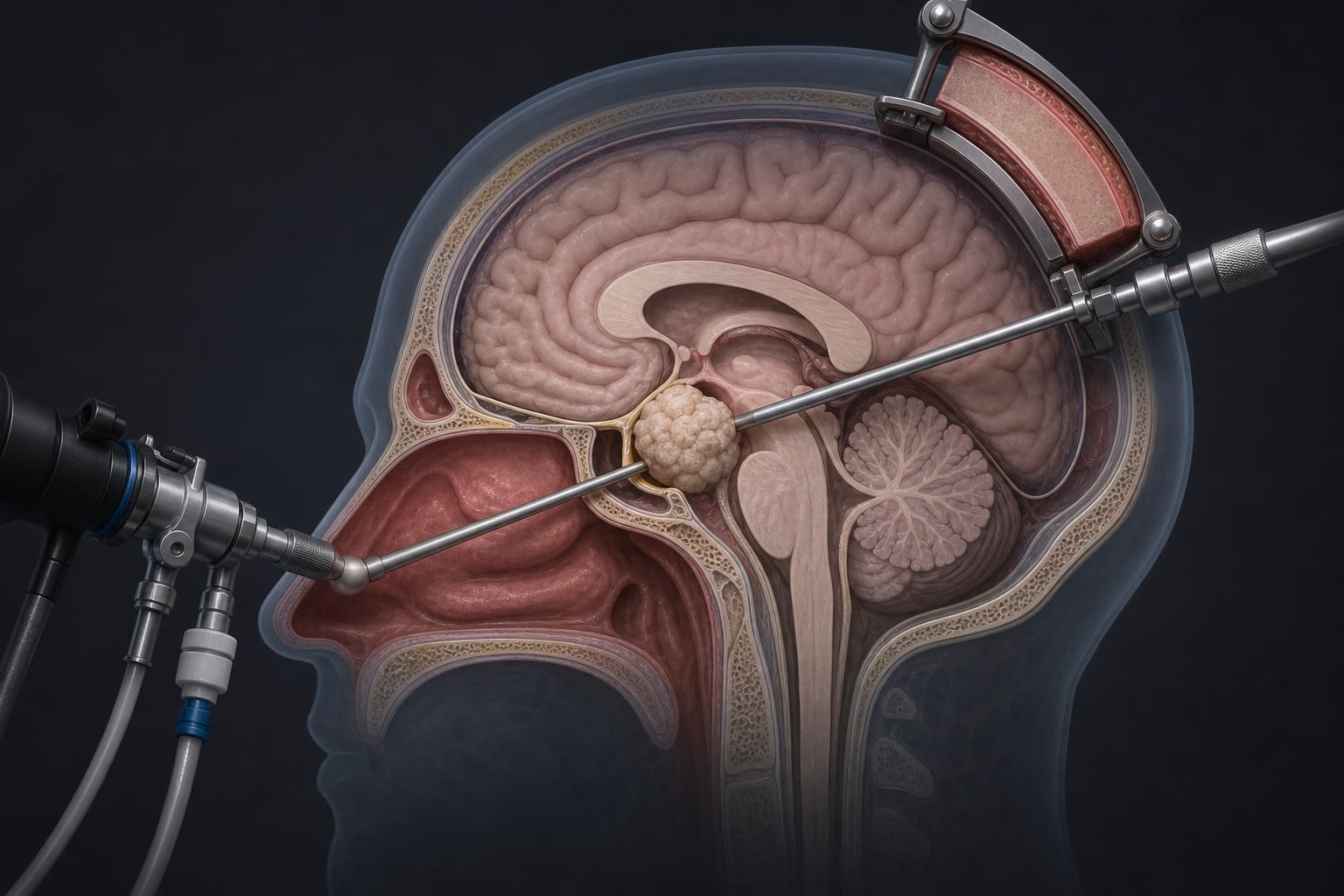
Treatment Strategies: Outlines microsurgery as the main treatment for CCJ AVFs, noting its high obliteration rate, while endovascular treatment is applicable in select cases.
Key Findings:
CCJ AVFs are rare, comprising 1-2% of cranial or spinal AVFs.
Common manifestations include subarachnoid hemorrhage and venous hypertensive myelopathy.
Accurate angiographic characterization is crucial for classification and treatment planning.
Microsurgery is preferred due to its high obliteration rate and durability.
Prognosis varies based on presentation, lesion subtype, venous drainage pattern, age, and treatment-related complications.
Interpretation:
The natural history of CCJ AVFs remains incompletely defined, necessitating structured angiographic follow-up post-treatment.
Limitations:
The rarity of CCJ AVFs complicates comprehensive understanding and management.
Natural history and outcomes are not fully characterized due to limited data.
Conclusion:
CCJ AVFs present unique challenges in diagnosis and treatment due to their complex anatomy and variable clinical presentations.