Trends and disparities in deaths involving atherosclerotic cardiovascular disease and stroke-related conditions among U.S. adults, 1999–2025 - Summary - MDSpire
Advertisement
Trends and disparities in deaths involving atherosclerotic cardiovascular disease and stroke-related conditions among U.S. adults, 1999–2025
To evaluate national trends and disparities in mortality involving coexisting ASCVD- and stroke-related conditions among U.S. adults from 1999 to 2025.
Approach:
Study Design: Retrospective population-based study using the CDC WONDER Multiple Cause of Death database.
Population: Included adults aged ≥25 years.
Mortality Identification: Deaths identified when both ASCVD-related and stroke-related ICD-10 codes were documented on the same death certificate.
Data Analysis: Age-adjusted mortality rates (AAMRs) calculated per 100,000 using the 2000 U.S. standard population.
Key Findings:
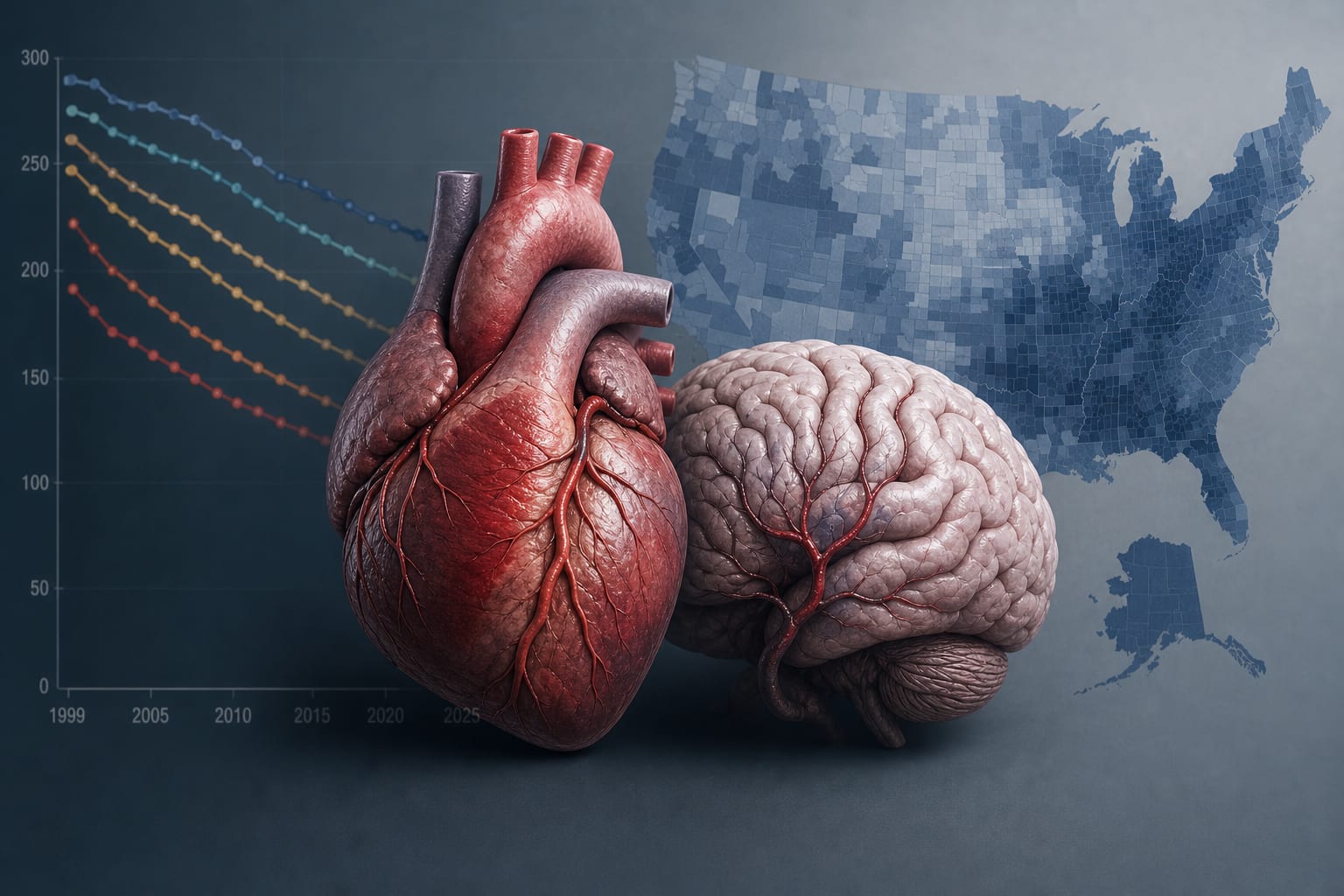
Total of 876,383 deaths identified with an overall average AAMR of 15.01 per 100,000.
Mortality declined from 26.82 in 1999 to 10.91 per 100,000 in 2025, with an average annual percent change (AAPC) of −3.53% (95% CI, −4.27 to −2.78; p < 0.001).
A borderline significant increase in AAMR was observed during 2018–2021 (APC: 6.06%; 95% CI, 0.01–12.48; p = 0.050).
Mortality burden remained higher among men, older adults, Black individuals, residents of the South, and non-metropolitan populations.
Adults aged 25–44 years showed a significant increase in mortality after 2015.
Interpretation:
Mortality involving coexisting ASCVD- and stroke-related conditions declined substantially from 1999 to 2025, but this progress was interrupted by a borderline reversal during the pandemic period and marked by persistent disparities.
Limitations:
Death-certificate data do not establish clinically adjudicated concurrent disease.
Analysis restricted to adults aged ≥25 years may overlook younger populations.
Conclusion:
Findings highlight the need for stronger and more equitable prevention strategies, particularly for younger adults and high-burden populations and regions.
A regional UK audit found wide variation in imaging intervals among patients referred for mechanical thrombectomy and identified potentially modifiable barriers to timely vascular imaging.